IJCRR - 6(2), January, 2014
Pages: 35-39
Print Article
Download XML Download PDF
FNAC STUDY OF MALE BREAST MALIGNANCY
Author: Parikh U.R., Dave P. N, Barot H.P., Goswami H.M., Jani H.U., Gonsai R. N.
Category: Healthcare
Abstract:Introduction: Although breast carcinoma is the second most common cause of death in female patients, male breast carcinoma is rare. The incidence for male breast carcinoma is about 1 % in all breast carcinoma. Clinicians also reported that the incidence of male breast carcinoma is increase day by day. Aims and Objectives: The present study was undertaken to determine the efficacy of FNAC in the diagnosis of these lesions. Material and Method: The present study was undertaken over a period of five months in one of the tertiary care teaching hospital. After detailed clinical history and examination, fine needle aspiration is performed in all the five patients. Result: Our 60 % of the patients are present in 7th decade. Total five male patients having malignant breast lesion on cytological examination. The cytological diagnosis is confirmed by histopathological examination. Discussion: Fine needle aspiration cytology is considered as a rapid diagnostic tool as well as it is reliable and less traumatic and is also able to differentiate non neoplastic and neoplastic breast lesions. This procedure is technically easy to apply in small breast lesions. FNAC is most accurate when experienced cytologists are available. The size and extent (stage) of tumors are the most important factors in the prognosis for male breast cancer. Conclusion: FNAC is outdoor patient procedure with high diagnostic accuracy, sensitivity and specificity.
Keywords: Fine Needle Aspiration Cytology (FNAC), Male Breast Cancer
Full Text:
INTRODUCTION
The role of fine needle aspiration cytology (FNAC) in male breast lesions has been reported in literature and is as reliable as in female breasts.1 Indeed, FNAC is the first line investigation in the clinical evaluation of breast lumps in males because it is a fast and cost effective method. It can be performed as an office procedure, requires little special equipment, causes minimal morbidity and has excellent patient acceptance. Breast cancer is the most common type of cancer in women, age 40 – 50 years. It is the second leading causes of cancer deaths i.e about 250,000 women die of this disease every year. 2 Men also possess a small amount of nonfunctioning breast tissue (breast tissue cannot produce milk) that is concentrated in the area directly behind nipple on the chest wall. Like breast cancer in women, cancer of the male breast is the uncontrolled growth of the abnormal cells of this breast tissue. 3 Male breast cancer is a rare condition, accounting for only about 1 % of all breast cancers.3 Most of the cases of male breast cancer are detected in men between the age of 60-70 years.3 The incidence of malignant neoplasia of male breast is on the rise. The apparent significant increase in the incidence is most probably attributable to an increase in screened cases and to increase awareness. The statistical significance coupled with decreased morbidity and mortality associated with early detection of malignant tumours. 2
MATERIAL AND METHOD
A detail study of five cases over a period of five months i.e. from April, 2012 to August, 2012 was carried out to determine the diagnostic accuracy of FNAC for male breast carcinoma, in pathology department of our tertiary care teaching hospital. After detailed clinical history and physical examination, aspiration was carried out using 22 gauge needle and standard precautions. Smears were immediately fixed in 95% ethyl alcohol. Smears were stained with May Graunwald Geimsa (MGG), Hematoxylin and Eosin stain (Hand E) and Papanicolaou (PAP) stain. Cytopathological diagnosis had been recorded in each case. Results of FNAC are confirmed by histopathological examination
RESULTS A
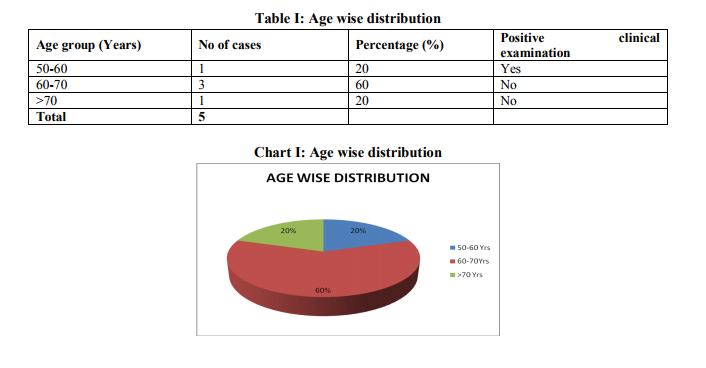
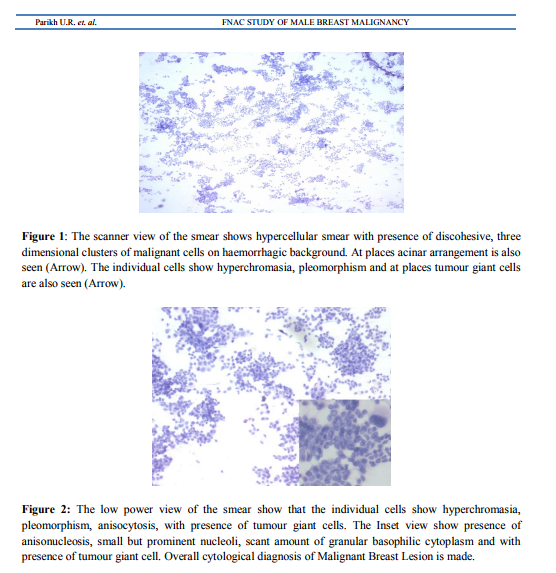
total of five patients with male breast lump have been diagnosed and treated at our tertiary care hospital over a period of five months i.e. from April, 2012 to August, 2012 are taken into consideration. In all the cases, detailed clinical examination and pre-operative FNAC has been done and diagnosis has been recorded. The FNAC report has been confirmed by histopathological examination in all the five case. Out of all patients, one of the patients is in 6th decade, three patients are in 7th decade and one patient is in 8th decade (Table I and Chart I). One of the patient (patient is in 6th decade) has history of ulceration and reddening of overlying skin with serous discharge from it. Four of our patients has lump of about 2 X 2 cm diameter, firm, well defined, immobile, non-tender and fixed to chest wall. Only one patient in 8th decade has lump of about 0.8 X 0.8 cm, firm, well defined, immobile, non-tender and fixed to chest wall. Axillary lymph nodes are not palpable in any of the above patients. No history of mumps orchitis in their younger age, testicular trauma or prostatic lesion has been found out. After taking consent, fine needle aspiration (FNA) is performed in all the five patients from two different sites and cytological examination is performed in H and E stained smears. The smears are hypercellular showing loosely cohesive three dimensional clusters, syncitial grouping of cells with absence of bipolar naked nuclei (Figure I). The individual cells show hyperchromasia, pleomorphism, anisocytosis, irregular nuclear border, small prominent nucleoli, and scant amount of coarsely granular basophilic cytoplasm with presence of abnormal mitotic figures (Figure II). Cytological diagnosis of malignant breast lesion is concluded in all the five cases. The diagnosis is confirmed by histopathological examination
DISCUSSION
Fine needle aspiration of the breast is a rapid, relatively atraumatic and accurate method for the diagnosis of breast disease.4 The real challenge for FNA cytologist is in their ability to translate cytological patterns into histological ones that have diagnostic meaning. Early diagnosis of cancer is crucial, a delay in the diagnosis of breast cancer is unfortunately common because of economic and social reasons in our society, with a poor impact on the management of such patients, it is therefore, important that a reliable cost effective and easy to perform investigation like FNAC should be done in such circumstances. A definite diagnosis sometimes cannot be made by FNAC either due to inherent limitations of cytological examination or by inability to obtain adequate material for diagnosis. The rate of sampling error and inadequacy for lesion < 1 cm can be attributed to deep location of the lesions.2 Male breast carcinoma represents 1% of all breast carcinomas in USA, but in countries like Egypt, the incidence raises to nearly 10%.5,6 One report from King Faisal Hospital in Taif KSA, breast carcinomas constituted 8.3%.6 A similar higher incidence of male breast carcinoma has been reported by Koriech.7 Though there are no recognizable etiological reasons and the higher incidence may be related to the higher incidence of liver cirrhosis following hepatitis B, leading to hyperestrinism and malignancy in susceptible males. 6 Our 60 % of the patients were in seventh decade which was correlated with Wick MR8 et al. A study published from the US Virginia Medical School calculated the mean age for ductal carcinoma in males at 64 years and they found that 60% of these patients were obese.8 Most of the breast carcinoma are treated by surgery. A modified radical mastectomy is most common surgical treatment for male breast cancer. After surgery, adjuvant therapies are often prescribed. Adjuvant therapies include chemotherapy, radiation therapy, targeted therapy, and hormone therapy.3 The prognosis of male breast cancer is similar to female breast cancer. As in women, the size and extent (stage) of tumors are the most important factors in the prognosis for male breast cancer. Overall survival rates for each tumor stage are similar for men and women. Since men have least breast tissue than women, it is more common for breast cancers in men to have spread beyond the breast when they are identified, resulting in a more advanced tumor stage at diagnosis.3 Disease-specific five-year survival rates (meaning the percentage of patients who do not die of the disease for at least five years following diagnosis) reported for male breast cancers by stage is as follows: ? Stage 0 – 100% ? Stage I - 96% ? Stage II – 88% ? Stage III – 60% ? Stage IV – 23% These survival rates were calculated using historical data, and it is likely that current treatments will lead to even greater survival rates for those recently diagnosed. FNAC is an efficient tool for diagnosing male breast lesions with high sensitivity and specificity and should be used confidently as an investigation of choice for diagnosing male breast lesions.
CONCLUSION
In this era of economic constraints, low allocation of health budgets in developing countries, lack of screening programs and increasing cost of diagnostic procedures, patients are invariably at a disadvantage and present late for medical assistance. It is, therefore recommended that FNAC should be used as a routine diagnostic procedure in rare lesions due to its cost effectiveness, thus maximizing the availability of health care to patients. Palpable breast lesions can definitely be diagnosed by a combination of physical examination and FNAC which when performed by a dedicated cytopathologist should be an integral part of a breast screening service. Thus, FNAC is useful to diagnose carcinoma in early stages which also improve the prognosis of the patients.
References:
REFERENCES
1. Ibrahim Mansoor, Awatif Jamal; The Value of Fine Needle Aspiration Cytology in the Diagnosis of Male Breast Lesions; Kuwait Medical Journal; 2001; 33 (3): 216-219.
2. Rakhshindah Bajwa And Tariq Zulfiqar; Association of fine needle aspiration cytology with tumor size in palpable breast lesions; Biomedica Vol.26, Jul. – Dec. 2010; P. 124 – 129
3. Chapter in book: Carcinoma of the Male Breast. Paul Peter Rosen; Rosen’s Breast Pathology; 2nd Edition; Lippincott Williums and Wilkins: 713-728.
4. McManus DT and Anderson NH. Fine needle aspiration cytology of the breast. Current Diagn Pathol 2001; 7: 262-271.
5. El Gazareyli M, Abdel Aziz AS. On bilharziasis and male breast cancer in Egypt. A preliminary report and review of literature. Br J Cancer. 1963; 17:566-571.
6. Ram Kumar G, Al Misiri S. (Letter to editor) Pattern of breast diseases in Saudi Arabia. Saudi Medical J 1997; 20:200-201.
7. Koriech OM, Profile of cancer in Riyadh Armed Forces Hospital. Annals Saudi Med 1994; 17:187-194.
8. Wick MR, Sayadi, Ritter JH, Hill DA, Reddy VB, Gattuso P. Low-stage carcinoma of the male breast. A histological, immunohistochemical, and flow cytometric comparison with localized female breast carcinoma. Am J Clin Pathol. 1999; 111:59- 69.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





