IJCRR - 6(23), December, 2014
Pages: 49-53
Date of Publication: 10-Dec-2014
Print Article
Download XML Download PDF
STUDY ON PATTERN AND MECHANISM OF ROAD TRAFFIC INJURY IN HOSPITALISED INJURY VICTIMS AND ITS ICD CLASSIFICATION
Author: P. Subhas Babu, T. S. Ranganath
Category: Healthcare
Abstract:Objectives: To stratify the different categories of road users sustaining Road traffic Injuries and admitted to Victoria hospital, Bangalore and to classify the Road traffic Injuries according to ICD-10th classification of diseases.
Methods: Cross Sectional, Hospital based descriptive study, conducted in Victoria Hospital, attached to Bangalore Medical College and Research Institute, Bangalore. All Road Traffic Injury Victims admitted as inpatients at Victoria Hospital from 1st April 2006 to 31st March 2007 were the study population. Cases were interviewed using purposive sampling method. A semi structured questionnaire, developed and standardized after initial pilot study, was used to capture study variables. Available medical records and MLC register were also used to collect and corroborate information. Study sample was 866 based on availability of victims of RTI. Results and Discussion: 866 patients were interviewed of the total 1409 patients who were admitted to the hospital during the study period. Majority of the victims were in the age group of 15 to 50 years (77.7%), with 25-39 years (35.1%) most affected among this group. 88.8% of the victims were males with 11.2% of them being females. Majority of the victims were two wheeler occupants (riders or pillions) ICD 10 code V20-V29 and pedestrians ICD Code V01-V09 constituting 34.2% and 31.6% respectively. Conclusion: Majority of the victims being in the productive age group, places an economic burden on the family. Among the road users injured majority of them are two-wheeler users and pedestrians and are vulnerable road users along with cyclists.
Keywords: ICD classification, Road traffic injuries (RTI), Vulnerable road users
Full Text:
INTRODUCTION
Deaths due to RTIs are among the 2 to 6th leading causes of death in the age groups within 5-60 years. During 1975-1998 mortality attributed to RTI increased by 79% in India, 237% in Columbia, 243% in China and 384%in Botswana. 1 In India the reported number of deaths due to Road “Accidents” were 80,262 in 2001, 84059 in 2002 and 84430 in 2003.2,3 The Integrated Disease Surveillance Programme highlights that Road Traffic Injuries are the sixth leading cause of death in India (IDSP-2005).4 Certain categories of road users like pedestrians, cyclists and motorized two wheeler users are more vulnerable to road traffic injuries, which has been found from studies conducted in major cities like Bangalore, Delhi and Puducherry.5,6,7 Uniformity in recording of category of road users injured in road traffic injuries and mechanism of injuries sustained ensures comparison of injury data across various settings and identifying specific intervention measures. The International Classification of Diseases – 10th revision is a useful tool for recording of Road traffic Injuries which are classified as external causes of Morbidity and mortality under transport accidents. The classification extends from V01-V99 and is structured in 12 sub groups.
OBJECTIVES
1. To identify the different categories of road users sustaining Road traffic Injuries and admitted to Victoria hospital, Bangalore.
2. To classify the Road traffic Injuries according to ICD-10th classification of diseases
METHODOLOGY
Study Design: Cross Sectional, Hospital based descriptive study. Setting: Victoria Hospital, attached to the Bangalore Medical College and Research Institute, Bangalore. The Hospital is a referral centre catering to the needs of people from different strata of society, but predominantly to lower and lower middle class. The Hospital is a reference centre for almost the whole of Bangalore Urban and Rural districts. Study population: All Road Traffic Injury Victims seeking care at Victoria Hospital as inpatients. Sample Population: Victims of Road Traffic injury, admitted to Victoria Hospital. Cases were interviewed on all days including on Sundays and Holidays. Purposive sampling method was used and those cases which were present at the time of the visit (between 8.00 am to 6.00pm) to the Hospital were interviewed.
Exclusion criteria
• Victims brought dead due to road traffic injuries.
• Victims who were immediately referred to higher centre.
• Victims who did not consent to be a part of the study.
Data collection tools: A semi structured questionnaire, developed and standardized based on an initial pilot study, to capture study variables. Available medical records and MLC register. Study duration: From 1st April 2006 to 31st March 2007. Statistical methods: Frequencies and proportions Data analysis: Data sets were coded and Windows® ExcelTM spread sheet, was used for data entry and analysis. The Study The study was carried out between April 1, 2006 and 31st March 2007 after obtaining clearance from the Institutional Ethics Committee of Bangalore Medical College and Research Institute. Patients were visited in the emergency wards, casualty, orthopedic and surgery wards. The victims were interviewed after obtaining an informed consent. When the condition of the patients did not permit the interview, the parents, relatives or attendants were interviewed. The information collected consisted of patient identification data, time day and class of vehicle involved in the Road Traffic injury, protective gears worn and category of road user. In addition, the type and severity of injury suffered by the victims was also recorded using the data collection tool.
OPERATIONAL DEFINITIONS
Injury The word injury as defined by Baker et al “…….. is the transfer of one of the forms of Physical energy (mechanical, chemical, thermal, etc) in amounts or at rates exceeding the threshold of human tolerance. And the term accident is to be used in the exceptional event of describing a primary event in a sequence that leads ultimately to injury if that event is genuinely not predictable. 8 Recent reports have indicated that deaths are under reported by 5-10% and injuries are under reported by more than 50% in police records. Persons injured in road accidents occupied nearly 10-30% of beds in the hospitals.9 Road Traffic Injury: It has been defined as injury which took place on road (including the side walk or foot path) between two or more objects, one of which must be any kind of a moving vehicle.10
Definitions for identifying different “accidents11
1. A transport accident (V01- V99) is any accident involving a device designed primarily for or being used for conveying persons or goods from one place to another 2. Other definitions like public highway (traffic way) or street, a roadway, pedestrian, driver, passenger, person on outside of vehicle, A pedal cycle, A pedal cyclist, A motorcycle, A motorcycle rider, A three-wheeled motor vehicle, A car (automobile), A pick up truck or van, A heavy transport vehicle, A bus, A special vehicle were obtained as per the ICD – 10 classification of external causes of mortality and morbidity. 3. Traffic accident (injury) is any accident occurring in the public highway (i.e. is originating on, terminating on, or involving a vehicle partially on the highway.) A vehicle accident is assumed to have occurred on the public highway unless another place is specified, except in the cases of injuries involving only off road motor vehicles, which are classified as non-traffic injuries unless the contrary is stated. 4. A non-traffic accident is any vehicle accident that occurs entirely in any place other than a public highway.
Categorization of Road Traffic Injury
Road Traffic Injuries are classified under land transport accidents (V01-V89) which reflect the victim’s mode of transport and are subdivided to identify the victim’s counterpart or the type of event. Sub-classification of the injuries has not been made in this study.
The vehicle of which the injured person is an occupant is identified in the first two characters since it is seen as the most important factor to identify for prevention purposes. The International classification of diseases (ICD 10) classifies road traffic injuries according to external causes of morbidity and mortality from code V01 to V89 in chapter XX and injury consequences of external causes from code S00 to T14 in chapter XIX.11
RESULTS AND DISCUSSION
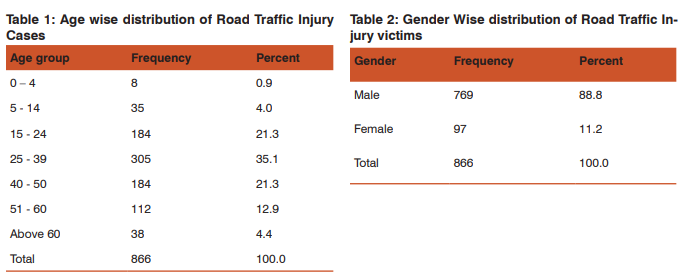
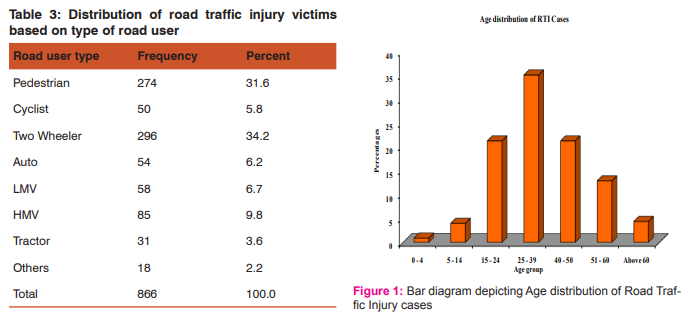
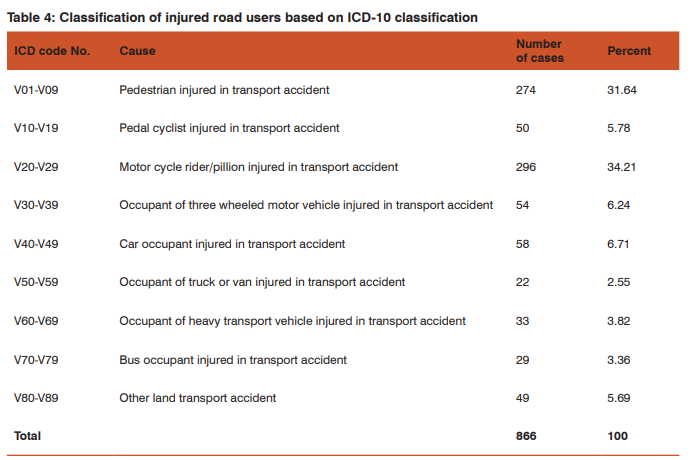
A total of 1409 patients were admitted during the study period, but only 866 patients could be interviewed as the casualty could not be visited on 24 hour basis and because of referrals. As evident from Table 1 and Fig 1, majority of the victims were in the age group of 15 to 50 years (77.7%), and 25- 39 years (35.1%) being most affected among this group. Children less than 14 yrs and elderly (>60yrs of age) made up a little under 5% each. According to the study done by Nilamber J et al in JIPMER7 maximum injuries were in the age group of 20-29 years (31.3%) and 71% of the victims were under 40 years of age. In another hospital based study by Ganveer GB10 majority of the victims were in the age group 18-37 years. In the study conducted at NIMHANS by Gururaj G et al5 highest number of Traumatic Brain Injuries with Road Traffic Injury was in the age group of 21-35 years (43%) with a male to female ratio of 4:1. This finding is in agreement with various studies which have found out that most of the victims are in their most productive agegroups. In the study done in the Municipal Corporation of Delhi6 of the total injuries 69% occurred in the age group of 15 to 35 years and males were four times more affected than females. It is evident that the victims are predominantly from a productive age group with the Road Traffic Injury resulting in a compromise in their quality of life. As evident from table 2. 88.8% of the victims were males with 11.2% of them being females. According to the study done by Nilamber J et al in JIPMER7 study 83% (603) were males and 123 (85.8%) were females. The central India study carried out by Ganveer GB10 found that 85.8% were males and 14.2% were females. Male to female ratio being 6:1. As males are more exposed to driving and go out for work they are at a higher risk of sustaining a RTI. In the study done in the Municipal Corporation of Delhi6 of the total injuries 69% occurred in the age group of 15 to 35 years and males were four times more affected than females. This difference may probably be due to the reason that males tend to travel more for work related and other purposes. As evident from table 3, majority of the victims were two wheeler occupants (riders or pillions) and pedestrians 34.2% and 31.6% respectively. Occupants of Auto and Light Motor vehicles made up 6.2% and 6.7% respectively. Occupants of Heavy motor vehicles accounted for 9.8% of the victims. Cyclists accounted for 5.8% of the victims. Rest of them were made up by occupants of tractors 3.6% and other vehicles 2.2%. According to the NIMHANS5 study 26% of the victims were pedestrians, 31% of them were two-wheeler riders 12% of them were two-wheeler pillions, 8% of them were bicycle users and passenger were 5%. As evident from table 4, majority of the victims were two wheeler occupants (riders or pillions) ICD 10 code V20-V29 and pedestrians ICD Code V01-V09 constituting 34.2% and 31.6% respectively. According to a community based study done by Pramod KV and Tewari KN in Delhi6 majority of the victims were Two-wheeler users 46.3% (315) and pedestrians 24.9%(169), followed by cycle users (14.1%), In the JIPMER7 study pedestrians constituted 22%, drivers (35%) and occupants of vehicles (45%) among the different type of vehicles 38.6% were bicycle users, 31.1% were motor cycle rides. Occupants of Buses (48%; 150) were the highest number of victims involved in Road Traffic Injuries, followed by truck occupants (12.6%).
CONCLUSION
Majority of the victims being in the productive age group, places an economic burden on the family apart from the physical pain and mental suffering. Among the road users injured majority of them are two-wheeler users and pedestrians. They are to be considered vulnerable road users along with cyclists. Pedestrian crossing needs to be increased and other road users need to be aware of pedestrians’ right of way. Though riders of vehicles have also suffered injuries, passengers (especially pillion riders on two-wheelers) are also vulnerable.
LIMITATIONS OF THE STUDY
1. Information is based entirely on the data collected from victims
2. As it is a Hospital based study it is not representative of the exact burden of Road Traffic Injury in the community.
3. Due to referral of cases to other institutions, some patients getting themselves discharged against medical advice and resource (time, single investigator) constraints not all victims could be interviewed.
ACKNOWLEDGEMENTS
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Ethical Clearance: The study was cleared by the Institutional Ethics Committee of Bangalore Medical College and Research Institute, Bangalore. Informed consent: obtained from all the subjects/ relatives who were interviewed (only those who consented were the study sample) Source of funding: The authors did not receive any funding from any external agency for the conduct of the study. Conflict of interest: The authors hereby declare that there is no conflict of interest with regard to this article and/or the research with which it is associated.
References:
1. Peden M, Scurfield R, Sleet D, Mohan D, Hyder A, Jarawan E, et al. World Report on Road Traffic Injury prevention. Geneva: World Health Organization; 2004 2. Accidental Deaths and Suicides in India. National Crime Records Bureau, Ministry of Home Affairs. Available from: http://www.ncrb.nic.in/ADSI2005 /accident05.pdf Accessed on, June 4th 2007.
3. Health Information of India-2004. New Delhi: Controller of Publications; 2005 (Directorate General of Health and Family Welfare).
4. Park K. Park’s Textbook of Preventive and Social Medicine. 19th ed. Jabalpur, India: M/s Banarasidas Bhanot Publishers, 2007; 340-345
5. Gururaj G, Kolluri SVR, Chandramouli BA, Subbakrishna DK, Kraus JF. Traumatic Brain Injury. Publication No. 61. Bangalore 560029, India: National Institute of Mental Health and Neurosciences; 2005: 17-23.
6. Pramod KV, Tewari KN. Epidemiology of Road Traffic injuries in Delhi: Result of a survey. Regional Health Forum. Delhi. WHO- SEAR 2004; 8 (1): 4-14.
7. Nilamber J, Goutam R, Jagadish S. Epidemiological study of road traffic cases: A study from south India. Indian Journal of Community Medicine 2004 Jan-Mar; xxix(1): 20-24
8. Barry PI, Brent EH. Injury Prevention: A Glossary of terms. J Epidemiol community Health 2005; 59: 182-185.
9. Health Situation in the South East Asian Region 1998- 2000, New Delhi: World Health Organization. Regional office for South East Asia, 2002: p 165-166.
10. Ganveer GB, Tiwari RR. Injury Pattern among non-fatal Road Traffic Accident cases: a cross sectional study in central India. Indian J Med Sci [serial online] 2005, [cited 2007 July 27]; 59(1), 9-12. Available from: http:// www.indianjmed.org/text.asp?2005/59/1/9/13812 Accessed on January 20th 2007.
11. International Statistical Classification of Diseases and Related Health Problems 10th revision.2nd ed. Geneva, Switzerland. World Health Organization; 2004.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





