IJCRR - 3(9), September, 2011
Pages: 37-41
Print Article
Download XML Download PDF
ANALYSIS OF ANTIBACTERIAL ACTIVITY OF CURCUMIN AGAINST ENTEROCOCCUS FECALIS
Author: Prasanna Neelakantan, Chandana Subbarao, Chandragiri Venkata Subbarao
Category: Healthcare
Abstract:Objectives: To evaluate the antimicrobial efficacy of curcumin against E. faecalis considering Sodium hypochlorite (3%) as references for comparison.
Methods: The antibacterial efficacy of a 100% pure solution of curcumin was evaluated against planktonic cells of E.fecalis using three tests: zone of inhibition, Minimum inhibitory and bactericidal
concentrations, and time taken to kill the cells, The data were statistically analysed by one-way ANOVA
and post hoc Tukey HSD test (p=0.05).
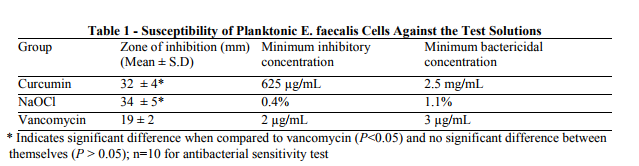
Results: The result revealed that curcumin had significant antibacterial activity against E.fecalis The zones of inhibition of curcumin against E.fecalis was 32 \? 4 mm, which was significantly different from
the standard - vancomycin, while the zone of inhibition for sodium hypochlorite was 34 \? 5mm. There
was no significant difference between the aforementioned data for sodium hypochlorite and curcumin (P
> 0.05) Tube dilution test revealed that MIC and MBC of curcumin were 625 \?g/mL and 2.5 mg/mL
respectively. While NaOCl, achieved 100% killing of E.fecalis at 2 minutes, curcumin was able to
achieve the same in 5 minutes.
Conclusions: The antibacterial activity of curcumin was similar to sodium hypochlorite . Considering the
potential for undesirable properties of NaOCl, the use of herbal alternatives in endodontics might prove to
be advantageous.
Keywords: Enterococcus faecalis, irrigant, phytotherapy, curcumin, sodium hypochlorite
Full Text:
Introduction
Root canal treatment (endodontic treatment) involves mechanical preparation of the root canal system, in conjunction with chemical aids. Although significant microbial reduction may be achieved by this, complete eradication of intra canal microbiota is unachievable using the currently used materials and techniques. Furthermore, it is well established that microbiota are the primary cause of pulp and periradicular pathoses 1 . Enterococcus faecalis, a facultative anaerobic gram-positive coccus, is the most common Enterococcus sp. cultured from non-healing cases 2,3. E. faecalis can adhere to the root canal walls, accumulate, and form communities organized in biofilm, which enables the bacteria to become highly resistant to phagocytosis, antibodies, and antimicrobials than non–biofilm-producing organisms 4,5. E. faecalis may also survive chemomechanical preparation, colonize within the intricate anatomical niches of the root canal system and reinfect the filled root canal 6 . Although the most commonly used and most effective chemical adjunct used in endodontics is sodium hypochlorite, this material has numerous disadvantages like unpleasant taste, toxicity, and potential weakening of the tooth structure by decreasing the hardness and structural integrity of the dentin within the root canal 7 . Medicinal plants represent a rich source of antimicrobial agents. Plants are used medicinally in different countries and are a source of many potent and powerful drugs. A wide range of medicinal plant parts is used for extract as raw drugs and they possess varied Medicinal properties. Recently, there has been a growing trend to seek natural remedies as part of dental treatment 8 . Two alternatives have been studied - Triphala (an Indian ayurvedic medicine) and Morinda citrofolia (Indian Noni) 9,10. However, these are not as effective as sodium hypochlorite. Turmeric (Curcuma longa) is extensively used as a spice, food preservative and coloring material in India, China and South East Asia. It has been used in traditional medicine for the treatment of numerous diseases. Curcumin (diferuloylmethane), the main yellow bioactive component of turmeric has been shown to have a wide spectrum of biological actions, including antimicrobial, anti-inflammatory and antioxidant activities 11,12,13. Many studies have attributed a wide spectrum of activities to this compound 14,15, and this provides a suitable basis for exploring its applications in dentistry, particularly in root canal treatment. It was the aim of the present study to analyse the antibacterial effect of curcumin against E.faecalis considering 3% sodium hypochlorite as reference for comparison. The null hypotheses was that there is no difference in the antimicrobial activity between curcumin and 3% sodium hypochlorite.
MATERIALS AND METHODS
A pure culture of E.faecalis (American Type Culture Collection 29212) was grown on Brain Heart Infusion agar. The microorganism was inoculated into tubes containing 5 mL sterile 0.9% saline solution. The suspension was adjusted spectrophotometrically at 800 nm to match the turbidity of 1.5 x 108 CFU/mL (equivalent to 0.5 McFarland standard) 16. Five hundred µL of each test microorganism suspension was used to inoculate glass bottles containing 50 mL BHI agar at 46°C, mixed and poured onto 130 mm plates containing a previously set layer of Mueller Hinton agar. The antibacterial activity of the test solution [Curcumin (Biopurify Phytochemicals Ltd.,Sichuan, China) and 3% sodium hypochlorite] was tested on planktonic cells using the antibacterial sensitivity test, tube dilution test and time to kill study. The absolute purity of curcumin (100%) was assessed by High Performance Liquid Chromatography (HPLC) prior to testing. Antibacterial sensitivity test: The antibacterial sensitivity test was performed by a standardised method described elsewhere 20. After drying the inocula, sterile filter paper discs (6-mm diameter) were applied using sterile forceps. One hundred microlitres of each material was pipetted onto the sterile paper disks. Ten replicates were prepared for each test solution. The plates were maintained for 2 hours at room temperature to allow diffusion of the agents through the agar and then incubated at 37°C for 24-48 hours in a carbon dioxide incubator (Jouan, Saint Herblain, France) in an atmosphere of 10% carbon dioxide. A standard vancomycin disc (30 mg) was included for comparison. Tube dilution method: Double dilution was made from a higher dilution of 100 mg/mL to a lower dilution in a series of test tubes. Each tube was inoculated with bacterial suspensions and incubated at 37°C overnight. The Minimum Inhibitory Concentration (MIC) was regarded as the lowest concentration in the series of dilutions, which did not permit the growth of the susceptible bacteria. The subcultures were made from the tubes which did not yield any visible turbidity in the MIC assay on freshly prepared Mueller-Hinton agar plates. After 24 hours of incubation at 37°C, the Minimum Bactericidal Concentration (MBC) was regarded as the lowest concentration of the test solution that allowed less than 0.1% of the original inoculum to grow on the surface of the medium. Test solutions were tested in triplicate (biological repeats) for each experiment. Analysis of time to kill: The bacteria [E. faecalis (ATCC 29212)] was exposed to the bactericidal concentration of the test solutions for 30 minutes. This was done by inoculating a loop full of the sample at regular intervals (2 minutes) on a Mueller-Hinton agar plate which was incubated at 37°C for 24 hrs, and observed for growth. The data were statistically analyzed by one-way analysis of variance and Student t test using SPSS software (SPSS Inc, Chicago, IL) with a significance level of 5%.
RESULTS
The zones of inhibition, MIC and MBC of test solutions are summarized (Table 1). The result revealed that curcumin had significant antibacterial activity against E.fecalis. There was no significant difference between the aforementioned data for sodium hypochlorite and curcumin (P > 0.05). While NaOCl, achieved 100% killing of E.fecalis at 2 minutes, curcumin was able to achieve the same in 5 minutes.
DISCUSSION
The present study compared the antibacterial activity of the predominant active component of turmeric ie., curcumin, against E.faecalis, the most resistant bacteria in root canal treatment. This appears to be the first report on the endodontic applications of curcumin. This material has shown antibacterial, antifungal and antiviral activity in previous studies 21,22,23. The MIC of curcumin against E.faecalis in this study was approximately 0.625 mg/mL, which is in accordance with an earlier report 24 . Components of turmeric are named curcuminoids [curcumin (diferuloyl methane), demethoxycurcumin, and bisdemethoxycurcumin]. These components are polyphenols with a strong antioxidant function 25. Curcumin, the most important fraction is responsible for the biological activities of turmeric. It has been hypothesized that curcumin inhibits the assembly of a protein - filamenting temperature-sensitive mutant Z (FtsZ) protofilaments and also increases the GTPase activity of FtsZ. The perturbation of the GTPase activity of FtsZ assembly is lethal to bacteria 26 . The results of this study showed that 3% NaOCl and curcumin achieved 100% killing of bacteria. albeit at different time intervals. However, this time difference is not significant in the clinical scenario, considering the potential drawbacks of sodium hypochlorite. The ability of 3% NaOCl to eliminate E.faecalis is in accordance with other reports 16,27. We speculate that Turmeric (curcumin) is able to eliminate the EPS matrix and the bacteria. This warrants further investigation. The concentration of curcumin that was effective against planktonic cells was 2.5 mg/mL. A higher concentration may be more relevant clinically, considering that bacteria form biofilms within the root canal system. Microbial communities in vivo are quite resistant to and difficult to eradicate with antimicrobials owing to the fact that the microorganisms to be targeted are organized in structures attached to each other and/or the root canal walls often involving a multitude of species known as microbial biofilms. The testing of antimicrobial agents against bacterial biofilms is yet to be standardized and no in vitro method accurately reflects the conditions under which microorganisms grow in vivo. So, caution should be exercised while extrapolating these results to the clinical scenario. A recent report suggested that curcumin in aqueous preparations exhibits phototoxic effect against gram positive and gram negative bacteria 28. This opens up avenues for further research on the use of turmeric in photodynamic therapy of root canal systems.
CONCLUSION
In conclusion, curcumin exhibited antibacterial activity similar to sodium hypochlorite and hence may be considered a viable alternative. Further research is warranted on this substance prior to clinical application as a root canal irrigant and intracanal medicament.
References:
1. Siqueira JF Jr, Rôças IN, Riche FN, et al. Clinical outcome of the endodontic treatment of teeth with apical periodontitis using an antimicrobial protocol. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008; 106:757–62.
2. Sundqvist G, Figdor D, Persson S, et al. Microbiologic analysis of teeth with failed endodontic treatment and the outcome of conservative re-treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;85:86–93.
3. Peciuliene V, Reynaud AH, Balciuniene I, et al. Isolation of yeasts and enteric bacteria in root-filled teeth with chronic apical periodontitis. Int Endod J 2001; 4:429–34.
4. George S, Kishen A, Song KP. The role of environmental changes on monospecies biofilm formation on root canal wall by Enterococcus faecalis. J Endod 2005; 31:867–72.
5. Kowalski WJ, Kasper EL, Hatton JF, Murray BE, Nallapareddy SR, Gillespie MJ .Enterococcus faecalis adhesin, Ace, mediates attachment to particulate dentine. J Endod 2006;32:634–37.
6. Ørstavik D and Haapasalo M. Disinfection by endodontic irrigants and dressings of experimentally infected dentinal tubules. Endod Dent Traumatol 1990;6:142–49.
7. Siqueira JF Jr., Rôças IN, Favieri A, Lima KC. Chemomechanical reduction of the bacterial population in the root canal after instrumentation and irrigation with 1%, 2.5% and 5.25% sodium hypochlorite. J Endod 2002;26:331–34.
8. Little JW. Complementary and alternative medicine: impact on dentistry. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004;98:137–45.
9. Murray PE, Farber RM, Namerow KN, Kuttler S, Garcia Godoy F. Evaluation of Morinda citrofolia as an endodontic irrigant. J Endod 2008;34:66 -70.
10. Prabhakar J, Senthilkumar M, Priya MS, Mahalakshmi K, Sehgal PK, Sukumaran VG. Evaluation of antimicrobial efficacy of herbal alternatives (Triphala and green tea polyphenols), MTAD, and 5% sodium hypochlorite against Enterococcus faecalis biofilm formed on tooth substrate: An in vitro study. J Endod 2010; 36:83 – 86.
11. Banerjee A, Nigam SS. Antimicrobial efficacy of the essential oil of Curcuma longa. Indian J Med Res 1978;68:864–866.
12. Goel A, Boland CR, Chauhan DP. Specific inhibition of cyclooxygenase-2(COX-2) expression by dietary curcumin in HT-29 human colon cancer cells. Cancer Lett 2001;172:111–118.
13. Srihari Rao T, Basu N, Siddqui HH. Anti inflammatory activity of curcumin analogues. Indian J Med Res 1982;75:574– 578.
14. Kumar V, Lewis SA, Mutalik S, Shenoy DB, Venkatesh, Udupa N. Biodegradable microspheres of curcumin for treatment of inflammation. Indian J Physiol Pharmacol 2002; 46:209–217. 15. Satoskar RR, Shah SJ, Shenoy SG. Evaluation of antiinflammatory property of curcumin (diferuloyl methane) in patients with postoperative inflammation. Int J Clin Pharmacol 1986;24:651–654. 16. Neelakantan P and Subbarao CV. An analysis of the antimicrobial activity of ten root canal sealers - a duration based in vitro evaluation. J Clin Pediatr Dent 2008;33: 31- 36.
17. Bauer AW, Kirby WWM, Sherris JC, Turck M. Antibiotic susceptibility testing by a standardized single disc method. Am J Clin Pathol 1966;45:493-496.
18. Bhavani Shankar TN, Sreenivasa Murthy V. Effect of turmeric (Curcuma longa) fractions on the growth of some intestinal and pathogenic bacteria in vitro. Indian J Exp Biol 1979:17:1363–1366.
19. Araujo CAC, Leon LL. Biological activities of Curcuma longa L. Mem Inst Oswaldo Cruz 2001;96:723–728
20. Jayaprakasha GK, Negi PS, Anandharamakrishnan C, Sakariah KK. Chemical composition of turmeric oil – a byproduct from turmeric oleorsin industry and its inhibitory activity against different fungi. Z Naturforsch C 2001;56: 40–44.
21. Ç?kr?kç? S, Mozio?lu E, Y?lmaz H. Biological Activity of Curcuminoids Isolated from Curcuma longa. Records of Natural Products 2008;2:19-24.
22. Chattopadhyay I, Biswas K, Bandyopadhyay U, Banerjee RK. Turmeric and curcumin: Biological actions and medicinal applications. Current Science 2004;87:44 – 53.
23. Rai D, Singh JK, Roy N, Panda D. Curcumin inhibits FtsZ assembly: an attractive mechanism for its antibacterial activity. Biochemical Journal 2008;410:147- 55
24. Giardino L, Ambu E, Savoldi E, Rimondini R, Cassanelli C, Debbia EA. Comparative evaluation of antimicrobial efficacy of sodium hypochlorite, MTAD, and Tetraclean against Enterococcus faecalis biofilm. J Endod 2007;33:852-855.
25. Kishen A, George S, Kumar R. Enterococcus faecalis-mediated biomineralized biofilm formation on root canal dentine in vitro. J Biomed Mater Res A 2006;77:406–415.
26. Simoés M, Pereira MO, Vieira MJ. Effect of mechanical stress on biofilms challenged by different chemicals. Water Research 2005;39:5142–52.
27. Chávez de Paz LE. Redefining the persistent infection in root canals: possible role of biofilm communities. J Endod 2007;33:652– 662.
28. Haukvik T, Bruzeli E, Kristensen S, Tønnesen H. Photokilling of bacteria by curcumin in selected polyethylene glycol 400 (PEG 400) preparations. Studies on curcumin and curcuminoids, XLI. Die Pharmazie 2010;65: 600-6.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





