IJCRR - 2nd Wave of COVID-19: Role of Social Awareness, Health and Technology Sector, June, 2021
Pages: 123-130
Date of Publication: 11-Jun-2021
Print Article
Download XML Download PDF
Breastfeeding During COVID-19 Pandemic in India: Challenges and Prospects
Author: Patnaik S, Jena D, Subudhi RN, Behera MR
Category: Healthcare
Abstract:Breastfeeding during infancy is important for good health and wellbeing. In India, rapid response to the COVID-19 pandemic resulted in lockdowns and limited or no mobility. As a result, Anganwadies (institutions supporting infant and young child feeding practices and supplementary nutrition) were closed for long durations. Frontline grassroots health workers such as ASHA (Accredited Social Health Activists), who also is responsible for promoting breastfeeding, were stretched with additional allocated work on COVID-19 rapid response. In India, myths around the transfer of COVID-19 from mothers to infants during breastfeeding did round. It is expected that the nutrition status of newborns and infants may have further worsened during COVID-19. Researchers have established that limited or no breastfeeding impacts the growth and development of infants during the critical first 1000 days also resulting in stunting. In this review we aimed to ascertain the status of breastfeeding practices during COVID-19 pandemic times and the impact it may have on infants. The objective of this article is to review the challenges and prospects of breastfeeding in India during the COVID-19 pandemic period. Through a review of literature, case studies, experience from on-ground rapid response to the COVID-19 pandemic, the current status of breastfeeding practices in India was reviewed. It may be concluded that there are many challenges as well as prospects for future pandemic preparedness and planning and to reduce risks addressing under-nutrition conditions of children such as stunting. A practical way forward maybe by using the suggested prioritization of States and interventions thereof based on stunting and breastfeeding status and efforts towards doing away with myths around breastfeeding.
Keywords: COVID-19, Breastfeeding, Stunting, Under-nutrition, Frontline Workers, Food Security
Full Text:
INTRODUCTION
Breast milk is an elixir for newborn babies and infants. It contains all important nutrients and antioxidants helping infants survive, grow and develop.1 UNICEF and WHO, recommend breast milk to be fed to a child within an hour of birth and exclusively for six months.2,3 The World Health Assembly’s 55th round declared that there is none next to breastfeeding as an ideal food for development and growth of infants, breastfeeding has implications on the reproductive health of mothers also, and that infant should be exclusively breastfed for the first six months for their optimal growth, development and health, this would be the global public health recommendation to be followed by all.4
Global Nutrition Report (GNR), 2020 indicates, India made limited progress towards achieving exclusive breastfeeding targets (58.0% infant aged 0-5 months breastfed). India is 'on course' to meet the target for stunting with 34.7% of children under 5 years stunted (higher than average for the Asia region: 21.8%).5 There is a need to address these gaps. If stunting is addressed effectively and given that it is “on course”, India can achieve being a nation free of at least one of the “nutrition burdens” i.e. “stunting”.6 In this scenario, development practitioners and frontline health workers shifted attention from nutrition towards rapid response to the COVID-19 outbreak.
Myths around the transmission of the disease while breastfeeding need to be dismissed as there is no evidence of transmission of disease from mother to baby or from breast milk consumption by a baby.7-11 UNICEF (2020), in its brief on Infant & Young Child Feeding (IYCF) during COVID-19, highlights that where episodes of diarrhoea, respiratory infections and infectious morbidity are common in babies, the possibility of risk of transmission of COVID-19 while breastfeeding is yet to be reported and that known risks associated with replacement feeding are far more devastating.12
At the same time, the production, marketing and sale of breast milk substitutes were found to be steady globally during the pandemic (Fortune Business Insights, 2020). Such products have been distributed to the needy by promoting them as instant food for infants and food security to vulnerable people impacted by COVID-19. A decline in breastfeeding practices is expected, unless, strong measures are taken to practice and promote it. Achieving SDGs for equitable health and nutrition will be a challenge, in this light.
The article aims to ascertain the status of breastfeeding practices during COVID-19 pandemic times and the impact it may have on infants. The objective of this article is to review the challenges and prospects of breastfeeding in India during the COVID-19 pandemic period. Information from the secondary review of literature, case studies, and experience from on-ground rapid response to the COVID-19 pandemic was used to ascertain the current status of breastfeeding practices in India during the ongoing pandemic period.
BREAST MILK: A NATURAL PREVENTIVE AND COMPLETE BABY FOOD
An irreplaceable food for a baby, breast milk helps in gaining muscular weight, mental agility, physiological functions, capacity to fight pathogenic infections and diseases and is a rich source of antibodies and antioxidants.13,14,15 Exclusive breastfeeding for the first six months of infants and breastfeeding within the first hour of birth is a preventive measure for numerous diseases, infections and unwanted health outcomes of infants/ children.1 The likelihood of infants dying is 14 times more if they have not been breastfed, as breastmilk consumption protects from sudden infant death syndrome, it also catalyses childhood development and higher intelligence, and lowers the risk of getting leukaemia, obesity or type-II diabetes.16 Breast milk during the first 1000 days of an infant provides a unique opportunity for its future holistic growth and development of physical and mental health.1
STATUS OF BREASTFEEDING IN INDIA
Worrisome to note that percentage change of children under the age of 5 years who are stunted shows a minimal decrease of 0.3% between the 4th and 5th National Family Health Survey (NFHS), despite budget allocation, initiatives by the Government and other development partners under “Poshan Abhiyan” (a Govt. of India nutrition scheme). Further between NFHS-4 & 5 (Figure 1), the % change in exclusive breastfeeding for children under age 6 months is in the negative (-2.1%). It is expected, that in 2020-21 during the ongoing COVID-19 pandemic, with decreased access to supplementary nutrition, mid-day meals and take-home rations, as well as limited counselling on nutrition and breastfeeding practice by frontline health workers as a result of lockdowns, norms of social and physical distancing, the status of stunting and exclusive breastfeeding practices would further decelerate. This calls for a special study specifically to ascertain the status of stunting and breastfeeding practices during the COVID-19 pandemic and a speedup of initiatives by prioritizing on States.17,18

Figure 1. Status of change in percentage of stunting, breastfeeding within the first hour of birth and exclusive breastfeeding between NFHS 3 (2004-05) and NFHS-4 (2015-16), and NFHS 4 (2015-16) & NFHS-5 (2019-20), Source: NFHS-3, 4, & 517-19
The NFHS-5 survey (2019-20) reports 99% institutional births, yet it is reported that only 46.9% of the children were breastfed within the first hour of birth. Additionally, 46.9% of the children under age 3 years that were breastfed within the first hour of birth as reported by the NFHS-5 (2019-20), was a marginal increase from NFHS-4 (2015-16) where the exclusive breastfeeding status was 41.9%.17,18
Ogbo et al.20 undertook a study in India to evaluate the prevalence of Exclusive Breastfeeding Practices (EBF) and found differing EBF practices from region to region. EBF practices were as high as 79.2% in Southern India, while it was 68% in North-Eastern India. EBF prevalence declined with infant age, declining faster in the South (about 44% at 5 months) as compared to that in the North-East region (54% at 5 months). Authors established, the association between higher maternal education with EBF in the Southern region, and an opposite association of same in the Central region of India, additionally, they found mothers from more wealthy households were less likely to engage in EBF in comparison with poorer households of Central India. A path-breaking study established that regional and local solutions are the need of the day and not an overall strategy for improving breastfeeding practices and overall nutrition outcomes of children.
Kumar et al.21 observed that under-fives were at a significantly high risk of under-nutrition whenever there were delays in initiating breastfeeding, colostrum deprivation and improper weaning, thus, optimal infant feeding practices must be promoted ad protected in this context.
The percentage change (decrease) in stunting between NFHS 4 & 5 (2015-16 and 2019-20) is found to be 0.9%. GNR (2020) indicates that India will miss the bus to achieving local nutrition targets by 2025 as India stands among those countries which have the highest rates of social and domestic inequalities and malnutrition.5,6,17,18
COVID-19 AND BREASTFEEDING CHALLENGES IN INDIA
There is no direct evidence as yet of transmission of the SARS-Cov-2 virus which causes COVID-19 disease from lactating mothers to breastfeeding infants7-11 although there are myths doing rounds. However, the indirect impact of COVID-19 could be manifold. On separation from a mother infected by the disease or a mother’s death because of the disease or any myths around breastfeeding during the pandemic, infants can be indirectly impacted. Food security issues during the lockdown period leading to poor health & nutrition of the lactating mother may result in the inability to produce enough milk. This needs further exploration.
While, ASHA workers have been appointed as the first point of contact for any health-related demands of deprived women and children, who find it difficult to access health services22, including the important role of creating awareness on determinants of health including nutrition and counselling women on prenatal and anti-natal care, safe delivery, breastfeeding, immunization etc. yet, during the lockdown period in 2020, ASHA workers could not function optimally because of social and physical distancing, lockdowns and limited access to protective gear. Although the Ministry of Home Affairs (MHA) informed that all essential services would be functional across the country, additional responsibility was given to them for rapid response to COVID-19 by tracking COVID-19 transmission cases, thus diverting those from their core work. Thus, impacting nutrition and counselling on breastfeeding practices.23
Stakeholder consultations during rapid response to COVID-19 in Jagatsinghpur & Mayurbhanj district (Odisha) by Arupa Mission Research Foundation (AMR, 2020) to address food security and safety of the community, frontline workers (ASHA, Anganwadi) and elected representatives during the peak pandemic period in 2020 and learning from the case study from Angul district of Odisha by Saigal (2020) indicate the following important points24: a) Absence of Take Home Rations (THR) for pregnant & lactating women for initial two-three months; b) Messaging and counseling on breastfeeding or nutrition by ASHA and Anganwadi workers took a backstage as focus was on COVID-19; c) Clarification on myths around transmission of COVID-19 disease from lactating mother to breastfeeding infant in both urban and rural areas was not done clearly; d) Families feared to receive THR as they felt it may lead to transmission of disease; e) Lockdown and fear of disease left some children of reversed migrants and migrants nutritionally vulnerable; and f) Focus of elected representatives, local governance bodies and CSOs was more towards food security for other vulnerable groups including migrants, and elderly, and contact tracing of super spreaders of COVID-19 disease; not on nutrition of infants.
Kumar et al.21 surveyed 1292 mothers who delivered in rural Mysore Block of South India between 2008 and March 2011. They found the following: firstly, 23.7% of mothers felt that they did not have enough breastmilk and this was the most common reason cited by them for non-exclusive breastfeeding; secondly, 42.6% of non-exclusively breastfed infants were fed formula/animal milk and 18.4% were fed oil/ghee.
Food security was an issue during the COVID-19 pandemic and may have impacted the nutrition intake of lactating mothers. There were also myths around the transmission of COVID-19 from animal milk and dairy products. Both these factors may have led to poor breastfeeding practices and the onset of stunting. This needs to be explored. Bhatt26 reports that in Delhi, West Bengal and Jharkhand poor mothers and babies were donated milk substitutes during the pandemic, following which, Arun Gupta of Breastfeeding Promotion Network (BPNI), the Government’s appointee to monitor implementation of the ‘Infant Milk Substitute Act of 1992’25 which prohibits distribution and promotion of infant milk substitutes to children under two years of age, filed an action alert. The action alert was in the form of a public notification, “issued on the BPNI website and to the media, urging the central government to tell state authorities to stop acceptance and distribution of infant formula in pandemic relief. He also sent letters to the Ministry of Health & Family Welfare and the National Disaster Management Authority, highlighting the separation of mothers and babies in suspected and confirmed covid-19 cases in hospitals and asking for a committee to investigate formula companies that exploit the pandemic for commercial gain.”27
CAGR (Compound Annual Growth Rate) forecast for 2019 to 2025 baby food market size by-products is 13.5% with value projection being 33 billion USD in 22 geographies including India.29 Although India adopted ‘The International Code of Marketing of Breast milk Substitutes (the Code) 1981’28 and ‘The Infant Milk Substitutes, Feeding Bottles and Infant Foods (Regulation of Production, Supply and Distribution) Act, 1992’25 further amended in 200327, regulating production, supply, and distribution of infant milk substitutes, feeding bottles and infant food to protect/ enhance breastfeeding practices and regulated use of infant food, there is an evident spurt in baby food production worldwide. Thus the core objective of limiting the negatives of milk substitutes, its promotion and enhancing breastfeeding practices including exclusive breastfeeding is unmet. The aggressive baby food market in India, together with myths on breastfeeding during COVID-19 and the diverted role of frontline health workers to covid-19 rapid response, distribution of infant milk products to poor mothers instead of provisioning with a nutritious diet will certainly impact the breastfeeding narrative outcomes in India.29
WHO and UNICEF encourage women to continue to promote breastfeeding during the COVID-19 pandemic, even if mothers have confirmed or suspected being infected with COVID-19 and that the multiple benefits of breastfeeding prevail over the potential risks of illness associated with COVID-19, infant formula milk not being a safer or only option.30
PROSPECTS OF IMPROVING BREASTFEEDING DURING PANDEMIC
COVID-19 pandemic ushered in a new way of living. New strategies to improve breastfeeding practices and nutrition outcomes of infants are the need of the hour. No “one shoe fits all” formula for improving determinants of nutrition (including breastfeeding within an hour of birth and exclusive breastfeeding for six months) will be effective given the diverse Indian culture and geography. However, recommendations from nutrition experts have bright prospects to address concerns around breastfeeding and stunting. Direct and indirect impacts of COVID-19 on breastfeeding practices and infant nutrition needs to be unfolded.
Menon et al.,31 on their district?focused analysis of stunting considered breastfeeding within an hour of birth and EBF as immediate determinants of stunting in India and recommended that there was a need for nationwide prevention of stunting as well as resolving district level variations of critical determinants of nutrition as well as inequalities and childhood stunting highlighted that in the Indian context if breastfeeding education is imparted at every anti-natal checkup, then even mothers with less than 10 checkups can learn about the benefits of breastfeeding and its methods. In the context of the COVID-19 pandemic, myths and fears doing rounds during the pandemic need to be studied and a campaign to address these via breastfeeding education implemented.32
Myths and fears doing rounds during the pandemic need to be studied and a campaign to address these via breastfeeding education is needed. Ogbo et al.,20 stated that multidimensional efforts at national and sub-national level, dedicated financial allocation, appropriate policies need to be in place to address the regional variations in breastfeeding practices in India were much needed. Concerning the COVID-19 pandemic, regional variations in EBF practices during the ongoing pandemic needs to be studied and addressed.
American Association of Pediatrics11 emphasized that infants should be exclusively breastfed for the first six months of life and only fed infant formula which is fortified with iron in case human milk is not available at all. Thus in the context of COVID-19, when it is established that the disease is not transmitted through breastmilk, then myths on it should be dismissed and breastfeeding promoted.
NFHS 5 (2019-20) data has been released for 22 States and Union Territories (UTs) of India. Based on findings from the NFHS 5 for two indicators: stunting among children aged 0 to 5 years and 0 to 3 aged children having been breastfed within an hour of birth, States and UTs can be divided into low risk, medium risk and high risk. High-Risk States and UTs must have a robust programme to ensure breastfeeding practices are improved for better nutrition outcomes of infants, especially for reducing future stunting. The objective of this categorization is to consider stunting and limited or lack of breastfeeding practices as risks to infant and child nutrition which is detrimental to their growth and, which when coupled with the challenges that COVID-19 has posed with regards to access, services and myths, may be disastrous for the nutrition outcomes of children. It may be so that in the event of natural calamities or epidemics and pandemics infants and children under three years of age would be doubly vulnerable not because of the disease as much as because of access, consumption and practice of nutrition. The strategy also lays the ground for focusing initiatives based on State needs rather than a one shoe fits all strategy as given below:
Category 1: High-Risk States
Those States which have high stunting levels (36% to 66% or more, Figure 2) and the percentage of children under the age of 3 years breastfed within the first hour of birth varies between 0 to 35%. The Graph below indicates the same:
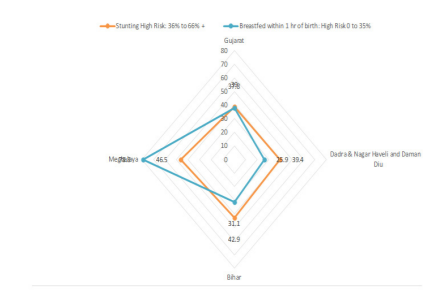
Figure 2. States with a high risk of stunted children 0 to 5 years and high-risk status of children in 0 to 3 years breastfed within an hour of birth (NFHS 5, 2019-20) in percentage.
According to the NFHS 5 data, Bihar has 42.9% of children in the age group of 0-5 years who are stunted, breastfeeding practice within an hour of birth is as low as 31.1% for children in the age group of 0 to 3 years and breastfed children exclusively breastfed for 6 months stands at 58.9 %. Similarly, two other critical States that need attention on priority are the Union Territories of Dadra & Nagar Haveli and Daman & Diu and the States of Gujarat, and Meghalaya. Meghalaya is an outlier, with a High proportion of stunting of children aged 0 to 5 years (46.5%) despite having a proportion of 0 to 3 year aged children breastfed within 1 hour of birth as high as 78.8%. The probability is that exclusive breastfeeding which is as low as 42.7% in Meghalaya, may be contributing to the stunting along with other factors. Meghalaya needs to be studied from the perspective of the impact
Category 2: Medium Risk States
Those States have the proportion of stunting varying from16% to 35% and the percentage of children under age 3 years breastfed within the first hour of birth varying from 36% to 66% (Figure 3). The States coming under the Medium Risk category include Andaman & Nicobar Islands, Kerala, Manipur, Goa, Jammu and Kashmir, Mizoram, Ladakh, Himachal Pradesh, Andhra Pradesh, Lakshadweep, Tripura, Nagaland, Telangana, West Bengal, Maharashtra, Assam and Karnataka. Sikkim is an outlier with a medium risk of stunting and a high risk of poor breastfeeding practices and would require special attention. The graph below indicates the same:
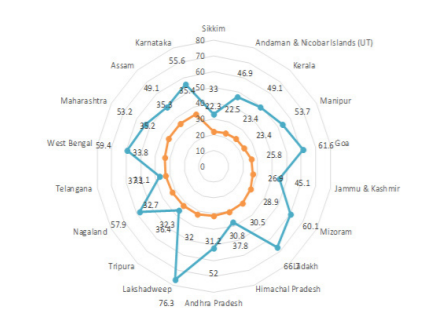
Figure 3. States with medium risk of stunted children in 0 to 5 years and medium risk of children in 0 to 3 years breastfed within an hour of birth (NFHS 5, (2019-20) in %
Category 3: Low-Risk States
Those States which have low stunting (0 to 15%) levels and the percentage of children under age 3 years breastfed within the first hour of birth varies from 67% to 100%. It may be noted that none of the States come under the low stunting category. However, the data for breastfeeding within an hour of birth is as high as 76.3% in Lakshadweep and 78.8% in Meghalaya. Given that Lakshadweep has 32% stunting, it has been included in the Medium Risk category and Meghalaya having 46.5% stunting has been included in the High-risk category.
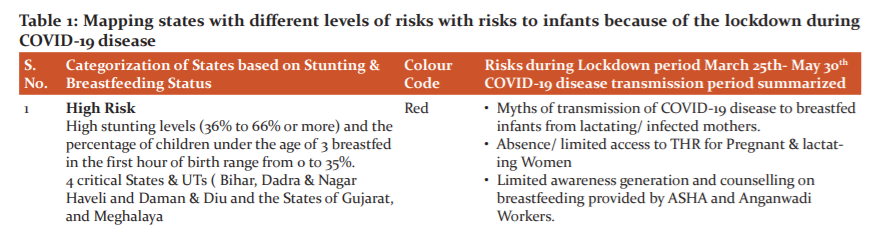
A robust plan by prioritization of States and UTs with separate strategies for high and medium risk States is the need of the hour especially in the light of the COVID-19 pandemic and its indirect impact on infants and children (Table 1). If we map the on the ground experience of the lockdown from 25th May 2020 onwards in India with the categorization of States based on stunting & breastfeeding as given in Table 1 below, we can correlate the risks to infants in the context of stunting and breastfeeding practices, as well as the level of risks.

As part of the prioritization strategy mentioned earlier, serious thought needs to be given to the risk to infant’s access to breast milk and nutrition because of limited counselling of mothers by frontline health workers during the pandemic and limited access to take-home rations. The fears and myths around COVID-19 and breastfeeding can be minimized through a focused campaign and behavioural change methods. Further, the need of the hour is also to conduct a nationwide study on the impact of the indirect impact of COVID-19 on breastfeeding practices and infants thereof. “Capacity Building and Training of Frontline workers on managing nutrition concerns and innovative ways of delivering roles and responsibilities during natural calamities, epidemics and pandemics.”23
Additionally, display of nutrition status at the Anganwadi and Panchayat Office. Mapping of nutritionally vulnerable children to be done, especially children of reverse migrants and migrants already present in the local area.23 Other to do’s include, provision on personal protection equipment to frontline workers, busting the myths around the transmission of COVID-19 disease through breast milk since research is ongoing and no evidence has been found as yet. Promotion of WHO and UNICEF norms for breastfeeding during the COVID-19 times, Participatory and interactive ICT based strategies for motivating working women and educated women to practice exclusive breastfeeding., Greater role to be played by Panchayats/elected leaders and civil society for addressing issues around the promotion of breastfeeding, stunting and COVID-19 preparedness and prevention in general and Effective implementation of the Food Security Act, especially for Take-Home Rations for pregnant and lactating mothers and the monitoring of the same.23
Importantly, the Government needs to put strict directives for regulation of the distribution of manufactured baby food during such episodes of disease outbreaks unless it is truly a need where natural breastfeeding is not an option. The messaging by manufacturers of baby food products needs to be monitored so that they don’t take advantage of such situations for their profits. Advocacy for stricter norms for the reduction in production, marketing, advertising and push selling of artificial infant formulas, baby food and milk supplements.23 The importance of having social and domestic support for mothers for sharing breastfeeding experience, voicing concerns and initiating mothers support groups at the community level (both rural and urban) as part of the strategy. For future studies, clear subject selection criteria and definition of “exclusive breastfeeding”, reliable collection of feeding data, controlling for important confounders including child-specific factors, and blinded assessment of the outcome measures will help.33 Empirical studies on breastfeeding practices during the COVID-19 pandemic will inform on minimizing risks to nutrition because of pandemics, relevant information for all stakeholders to design and implement effective strategies for better nutrition outcomes for India. Addressing the burden of stunting effectively, given that it is on course, India must at least work towards achieving being a nation free of at least one of the nutrition burdens which is “stunting” with political will, right strategies and proper implementation.
CONCLUSION
India is at a critical juncture about nutrition outcomes. It is expected that India will miss achieving nutrition goals unless need-based measures are taken. It is found that there can be no one she fits all solution to address the nutrition gaps in a country with diverse cultures ad ways of living. Further, with the COVID-19 pandemic, access to nutrition and nutrition-based services had become restricted. Also, there were many myths around breastfeeding practices and the spread of the disease. Baby food manufacturing companies are also taking advantage of the situation. Given these challenges, India still has prospects to be a nation free of stunted children if the right strategies and prioritization of initiatives for improving breastfeeding practices and reducing stunting are adopted. There is scope for further empirical studies on how and to what extent breastfeeding practices and nutrition were impacted in the country during the ongoing pandemic. This would also be important for improved future risk management and preparedness in such situations of pandemics. Recommendations for national, regional, district-level need-based interventions based on variations and prioritization of strategies for high, medium and low-risk States is critical.
CONFLICT OF INTEREST: None
SOURCE OF FUNDING: None
ETHICAL APPROVAL: Not applicable for this manuscript
ACKNOWLEDGEMENTS: The authors thank Nibal Dibiat for his sincere comment on the draft and formatting of the manuscript. Further, we appreciate the body of work by various scholars and acknowledge that their articles cited & referenced in this manuscript has been of immense help. We are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. National guidelines on infant and young child feeding. Ministry of women and child development (food and nutrition board) 2006. Available from: https://wcd.nic.in/sites/default/files/infantandyoungchildfeed.pdf
2. Unicef. Breastfeeding a mothers gift for every child. 2018. Available from: https://www.unicef.org/media/48046/file/UNICEF_Breastfeeding_A_Mothers_Gift_for_Every_Child.pdf
3. World Helath Organization. Global strategy for infant and young child feeding: the optimal duration of exclusive breastfeeding. Geneva WHO. 2001.
4. World Helath Organization. Infant and young child nutrition: global strategy on infant and young child feeding. Rep by Secr. 2002;
5. Micha R, Mannar V, Afshin A, Allemandi L, Baker P, Battersby J. Global nutrition report: action on equity to end malnutrition 2020. https://globalnutritionreport.org/reports/2020-glo...
6. Global Nutrition Report. The Burden of Malnutrition at a Glance [Internet]. Country Nutrition Profile, India. 2020. Available from: https://globalnutritionreport.org/resources/nutrition-profiles/asia/southern-asia/india/?country-search=India
7. Salvatore CM, Han J-Y, Acker KP, Tiwari P, Jin J, Brandler M, et al. Neonatal management and outcomes during the COVID-19 pandemic: an observational cohort study. Lancet Child Adol Heal. 2020;4(10):721–7.
8. Davanzo R, Moro G, Sandri F, Agosti M, Moretti C, Mosca F. Breastfeeding and coronavirus disease?2019: Ad interim indications of the Italian Society of Neonatology endorsed by the Union of European Neonatal & Perinatal Societies. Matern Child Nutr. 2020;16(3):e13010.
9. Chen H, Guo J, Wang C, Luo F, Yu X, Zhang W, et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: a retrospective review of medical records. Lancet. 2020;395(10226):809–15.
10. Guidance for Management of Pregnant Women in COVID-19 Pandemic. Indian Council of Medical Research. Natl Inst Res Reprod Heal 2020 Apr 05. https//www icmr gov in/pdf/covid/techdoc/Guidance_for_Management_of_Pregnant_Women_in_COVID19_Pa ndemic_12042020 pdf.
11. Breastfeeding guidance post-hospital discharge for mothers or infants with suspected or confirmed SARS-Co V-2 infection. Dostupno na https//services aap org/en/pages/2019-novel coronavirus-covid-19-infections/breastfeeding-guidance-post-hospital discharge/(Pristupljeno 2504 2020). 2020;
12. UNICEF. Infant and young child feeding in the context of COVID-19 [Internet]. Retrieved from the Emergency Nutrition Network (ENN) website: www. en online; 2020. Available from: aa9276_f45d1a6971154d5bb4b102a03877c28f.pdf.
13. Lönnerdal B. Breast milk: a truly functional food. Nutrition. 2000;16(7/8):509–511.
14. Li W, Hosseinian FS, Tsopmo A, Friel JK, Beta T. Evaluation of antioxidant capacity and aroma quality of breast milk. Nutrition. 2009;25(1):105–114.
15. Alimoradi F, Javadi M, Barikani A, Kalantari N, Ahmadi M. An overview of the importance of breastfeeding. J Compr Pediatr. 2014;5(2):461-464.
16. Organization WH. Marketing of breast-milk substitutes: National implementation of the international code, status report 2020: summary. In: Marketing of breast-milk substitutes: National implementation of the international code, status report 2020: summary. 2020.
17. National Family Health Survey (NFHS)-4. Minist Heal Fam Welf Gov India. 2015;(16). Available from: http://rchiips.org/NFHS/factsheet_NFHS-4.shtml
18. National Family Health Survey (NFHS)-5. Minist Heal Fam Welf Gov India. 2019;(20). Available from: http://rchiips.org/NFHS/NFHS-5_FCTS/NFHS-5 State Factsheet Compendium_Phase-I.pdf
19. National Family Health Survey NFHS-III 2005-06. Minist Heal Fam Welfare, Govt India. 2006;(6). Available from: http://rchiips.org/nfhs/factsheet.shtml
20. Ogbo FA, Dhami MV, Awosemo AO, Olusanya BO, Olusanya J, Osuagwu UL, et al. Regional prevalence and determinants of exclusive breastfeeding in India. Int Breastfeed J. 2019;14(1):1–12.
21. Kumar D, Goel NK, Mittal PC, Misra P. Influence of infant-feeding practices on nutritional status of under-five children. Indian J Pediatr. 2006;73(5):417–21.
22. GoI. SOP - Contact Tracing for COVID-19 Cases. National Center for Disease Control (Formerly National Institute of Communicable Diseases). Available from: https://ncdc.gov.in/index1.php?lang=1&level=1&sublinkid=632&lid=542 and https://ncdc.gov.in/showfile.php?lid=538
23. Patnaik S. Breastfeeding in COVID-19 times: Learnings and way forward. Curr Opin Virus Infect Dis. 2020;1(3):43–50.
24. Saigal N. Frontline COVID Warriors: A Lesson From Odisha. Outlook POSHAN. 2020. Available from: https://poshan.outlookindia.com/story/poshan-news-frontline-covid-warriors-a-lesson-from-odisha/350481
25. The Infant Milk Substitutes, Feeding Bottles And Infant Foods (Regulation Of Production, Supply And Distribution) Act. 1992. Available from: https://www.indiacode.nic.in/bitstream/123456789/1958/1/199241.pdf
26. Bhatt N. Breastfeeding in India is disrupted as mothers and babies are separated in the pandemic. Br Med J. 2020;370:m3316. doi: 10.1136/bmj.m3316.
27. The Infant Milk Substitutes, Feeding Bottles and Infant Foods (Regulation of Production, Supply and Distribution) Act, 1992 as Amended in 2003 (IMS Act). Available from: http://www.bpni.org/docments/IMS-act.pdf
28. World Health Organization. International code of marketing of breast-milk substitutes. World Health Organization; 1981.
29. Pulidindi K, Pandey H. Baby Food Market Size By Product (Prepared, Dried), By Distribution Channel (Hypermarket, Supermarket, Convenience Stores, Online), Regional Outlook, Application Growth Potential, Price Trends, Competitive Market Share & Forecast, 2019–2025. Global Market Insight. 2018; 250.
30. World Health Organization. Agencies encourage women to continue to breastfeed during the COVID-19 pandemic. News release, Geneva, New York; 2020. Available from: https://www.who.int/news/item/27-05-2020-countries-failing-to-stop-harmful-marketing-of-breast-milk-substitutes-warn-who-and-unicef
31. Menon P, Headey D, Avula R, Nguyen PH. Understanding the geographical burden of stunting in India: A regression?decomposition analysis of district? level data from 2015–16. Matern Child Nutr. 2018;14(4):e12620.
32. Nishimura H, Krupp K, Gowda S, Srinivas V, Arun A, Madhivanan P. Determinants of exclusive breastfeeding in rural south India. Int Breastfeed J. 2018;13(1):1–7.
33. Chung M, Raman G, Chew P, Magula N, Trikalinos T, Lau J. Breastfeeding and maternal and infant health outcomes in developed countries. Evid Techn Asses. 2007;153(153):1–186.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





