IJCRR - 6(4), February, 2014
Pages: 15-20
Date of Publication: 20-Feb-2014
Print Article
Download XML Download PDF
A RARE CASE OF EARLY PREGNANCY WITH PARAGANGLIOMA OF URINARY BLADDER
Author: Girija Malavalli Kempasiddaiah, Renuka Thimmaiah, Mallikarjuna Gurappa Desai
Category: Healthcare
Abstract:The paraganglia are the neuroendocrine tissues which are symmetrically distributed along the para vertebral axis from the base of the skull to the neck of the pelvis. Tumors of these paraganglia are called as Paraganglioma. It is a neuroendocrine tumor, majority of them are benign. Paraganglioma affecting the urinary bladder in pregnancy is extremely rare condition. An early diagnosis of Paraganglioma, in the 1st trimester will result in a good outcome, if treated by surgical intervention and these patients can be delivered vaginally instead of caesarean section.
Keywords: Paraganglioma, pregnancy, neuroendocrine, urinary bladder
Full Text:
INTRODUCTION
Paraganglioma is a neuroendocrine neoplasm, occurring at various sites in the body. 97% of paraganglioma are benign and 3% malignant neoplasm. Prevalence of paraganglioma in urinary bladder is <1% and associated with pregnancy is extremely rare1 . It arises from the chromaffin tissues of the sympathetic nervous system present in the wall of the urinary bladder. The spectrum of presentation varies from painless haematuria, hypertensive crisis, palpitations, anxiety, sweating and hot flushes2 .
CASE REPORT
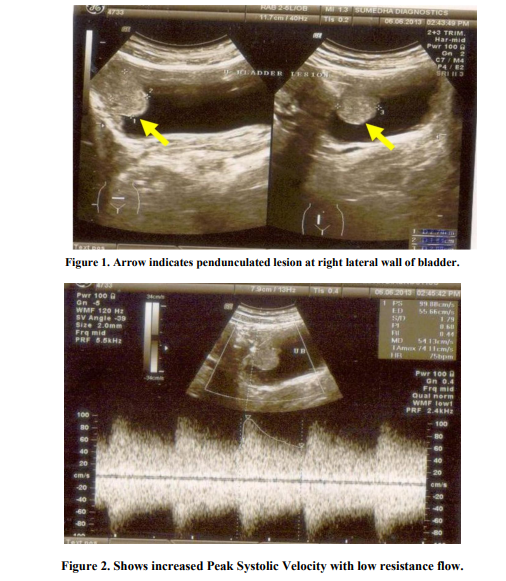
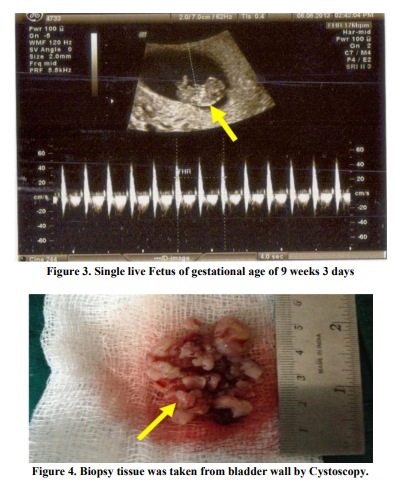
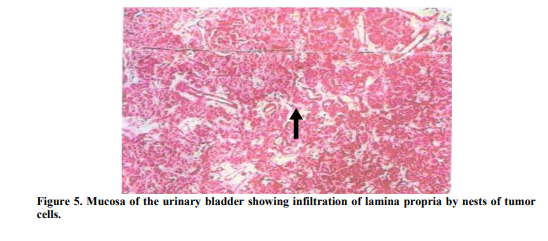
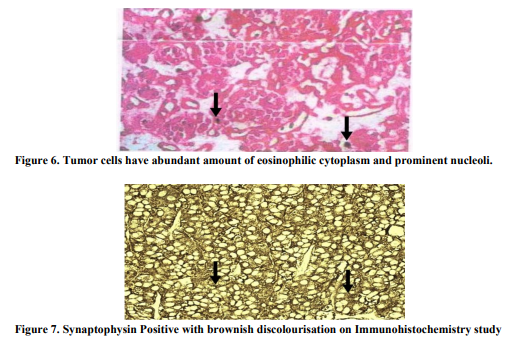
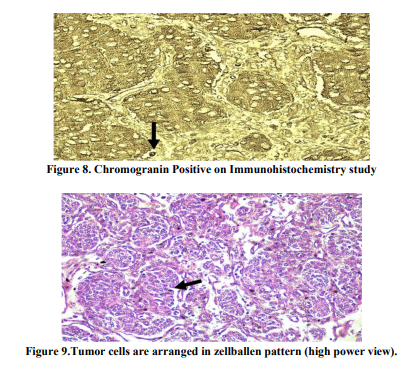
A 25 year old female, presented to our hospital with a history of painless haematuria on 5th June 2013, associated with fever and vomiting since 2 days. She was G2P1L1 with 9 weeks 2 days of gestation. Her Last menstrual period was on 24th April 2013. Fever was intermittent, low grade; no chills and rigor were present. She had 2-3 episodes of vomiting, non projectile and non blood stained. She had complaints of lower abdominal pain since 2 days which was intermittent, spasmodic and radiating to the back. Her past medical history were not significant. On General physical examination, she was febrile and mild pallor was present. Her pulse was 109 beats/ minute and Blood pressure was 100/64 mm of Hg. On Abdominal examination, the abdomen was soft, suprapubic tenderness was present and no organomegaly was found. Uterus was not palpable.On Bimanual examination, uterus was 8- 10 weeks, non tender and no bleeding per vaginum. Her hemoglobin level was 9.1 g/dl, White blood cell count was 9300/mm3 , Blood urea 14mg% and Serum creatinine 0.1mg%. Routine urine examination showed plenty of Red blood cells. Ultrasound report showed well distended Urinary bladder with normal wall thickness. There was a well defined pedunculated lesion seen arising from inner margin of right lateral wall of urinary bladder and projecting into the lumen, seen around 9’O clock position measuring about 31x32x23mm size (Figure1). There was increased vascularity seen with arteries showing increased Peak Systolic Velocity with low resistance flow pattern (Figure2). A Gravid uterus with a single live active embryo in a well defined intrauterine gestational sac with Crown Rump length 26mm corresponding to 9 weeks 3 days ± 1 week (Figure3). In view of the report, a urological opinion was taken and a cystoscopy was done, showing 3x2 cm pedunculated growth in the right lateral wall. Bilateral Ureteric orifices were normal. A complete transurethral resection of bladder tumor was done and was sent for histopathology (Figure4). Post Operative period was uneventful and patient well being was improved. Histopathology report revealed infiltration of the lamina propria by nests of cells in the bladder mucosa. These cells had abundant amount of eosinophilic cytoplasm and fairly uniform nuclei with vesicular chromatin and visible nucleoli. Areas of congestion and hemorrhage were seen. Mitotic activity was not increased, all the features suggestive of paraganglioma (Figure5&6). Immunohistochemistry was done for confirmation, which showed Synaptophysin (Figure7). Another Immunohistochemistry was done, which showed Chromogranin A positive (Figure 8). Other markers like c-kit (CD 56), Creatinine kinase (CK) and ki-67 were negative. Immunohistochemistry showed polygonal to oval tumor cells, arranged in distinctive cell balls, zellballen pattern (Figure9) which are separated by fibrovascular stroma and sustentacular cells.
DISCUSSION
Paragangliomas are the tumors which arise from the neuroendocrine tissues called as paraganglia. These paraganglia are symmetrically distributed in the body along the paravertebral axis extending from their predominant location at the base of the skull to the neck of the pelvis.3 Paragangliomas in the skull base, upper mediastinum and neck are primarily associated with the parasympathetic nervous system and generally do not hyper secrete catecholamines or other hormones. Only about 5% of skull base and neck paragangliomas hyper secrete catecholamines. Paragangliomas in the lower mediastinum, abdomen (85%), and pelvis are typically associated with the sympathetic nervous system and usually hyper secrete catecholamines.4 These tumors have chromaffin cells which refers to the brown black color resulting from oxidation and polymerization of catecholamines present in the cells/tumors having chromium salts.5 Paraganglioma associated with pregnancy may present with a spectrum of presentations: pre eclampsia, palpitations, sweating, pallor, orthostatic hypotension and glycosuria, and hypertension may be episodic.3 But in this present case, the patient came to us at her 1st trimester of pregnancy; the symptoms were not profound and striking. Surgery is the definitive treatment of choice for these tumors, with appropriate alpha-adrenergic, and if needed, subsequent beta-adrenergic blockade to prevent a hypertensive crisis. Phenoxybenzamine is the alpha blocker of choice in both pregnant and non-pregnant individuals with catecholamine secreting tumors. For intraabdominal paraganglioma, a laparoscopic surgical approach is ideal if the tumor size allows.5 After 24 weeks gestation, surgery may need to be delayed until fetal maturity is reached (~34 weeks) because of problems with tumor accessibility. An open surgical approach combined with elective caesarean section may need to be performed in these situations. A good outcome has only been described with vaginal delivery in selected cases.5
CONCLUSION
Urinary bladder paraganglioma although rare, should be included in the differential diagnosis of melanoma and carcinoid tumor. An early cystoscopy, if considered may help to diagnose this clinical entity. Our case is one of the rare case, as patient came to us with early pregnancy associated with bladder growth which was completely removed and confirmation was done with immunochemistry. The patient is now in her late 2nd trimester of pregnancy.
ACKNOWLEDGEMENT
My sincere thanks to Dr Desai M.G Dept of Surgery, for helping me in handling this case. The authors are also grateful to authors/editors/publishers of all those articles, journal and books from where the literature for this article has been reviewed and discussed
References:
1. Demirkesen O, Cetinel B, Yaycioglu O, Uygun N, Solok V. Unusual cause of early preeclampsia : bladder paraganglioma. Urology. 2000; 56(1):154.
2. Onishi T, Sakata Y, Yonemura S, Sugimura Y: Pheochromocytoma of the urinary bladder without typical symptoms. Int J Urol 2003, 10(7):398-400
3. Kirmani S, Young WF. Hereditary Paraganglioma-Pheochromocytoma Syndromes. 2008 May 21 [Updated 2012 Aug 30]. In: Pagon RA, Adam MP, Bird TD, et al., editors. GeneReviews™ [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2013. Available from: http://www.ncbi.nlm.nih.gov/books/NBK154 8/
4. Lee KY, Oh Y, Noh HJ, Lee YJ, Yong H,Kang E, Kim KA,Lee NJ. Extraadrenal Paragangliomas of the Body: Imaging Features. AJR 2006; 187:492-504.
5. Wald O, Shapira OM, Murar A, Izhar U. Paraganglioma of the mediastinum: challenges in diagnosis and surgical management. J Cardiothorac Surg. 2010; 5:19.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





