IJCRR - 6(24), December, 2014
Pages: 16-18
Date of Publication: 20-Dec-2014
Print Article
Download XML Download PDF
ISOLATED AND UNILATERAL DELAYED ONSET MUSCLE SORENESS AFFECTING GASTROCNEMIUS -MAGNETIC RESONANCE IMAGING VALIDATION AND TREATMENT
Author: Ganesh Singh Dharmshaktu, Irfan Khan
Category: Healthcare
Abstract:The Delayed onset muscle soreness (DOMS) is a response to musculoskeletal insult following bouts of extraordinary physiological overload. The condition can take a morbid course if neglected or undertreated. Often considered a primer for musculoskeletal reparative process, the phenomena should be managed with holistic approach. The presented case is an uncommon pattern of DOMS in common settings and its appropriate management. It also highlights the importance of preventive and rehabilitative aspect of the condition.
Keywords: Delayed onset muscle soreness, Magnetic resonance imaging, Physical therapy
Full Text:
INTRODUCTION
The Delayed onset muscle soreness (DOMS) results from intensive, unaccustomed eccentric muscle activity and is a cause of variable clinical presentation ranging from mild pain to severe morbidity.[1] Initiation of a sports or endurance activity especially after a period of inactivity is common cause. Usually a self limiting event can take a chronic course if not managed early. Usually the DOMS affects multiple muscle groups at the same time and isolated and unilateral involvement after physical endurance is an uncommon occurrence.
CASE REPORT
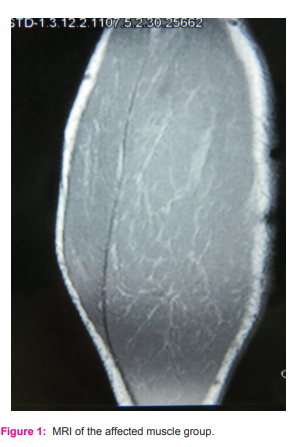
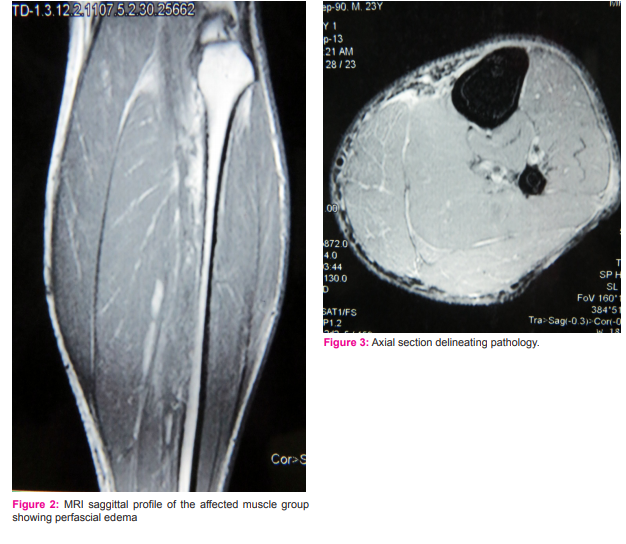
A 23 year old male presented to us with complaints of left calf pain that was mild and intermittent to begin with but gradually increasing in severity and duration. There was history of involvement in military recruitment camp two days back. There was history of intense physical exertion including drills, running and other physical tests during the recruitment drive. He was having mild but tolerable pain which he dismissed as a transient episode. The pain got intense by third day and the patient found unable to bear weight and ambulate with the affected limb. The pain was severe and affecting the activities of daily living. The patient consulted a local practitioner where he was advised some pain medication including muscle relaxant. He consulted us a day later after he found no relief with a short period of rest, limb elevation and medications. On clinical examination, the patient has spasm over his left upper calf muscle and relative localized swelling at painful area when compared to contra lateral limb. The affected calf and gastrocnemius muscle was tender. The local temperature was normal and there was no history of other ‘red flags’. The pain was localized, increased on use of the limb and without any referral pattern, radiation or diurnal variation. The provisional diagnosis of muscular spasm of calf was made and patient was admitted for supervised physical therapy and appropriate supportive management. Magnetic resonance imaging (MRI) was done by patient out of comprehension to rule out serious underlying disorder.(Fig. 1) The MRI correlated with DOMS affecting gastrocnemius region with myofascial edema in medial and lateral head of gastrocnemius with perifascial fluid.(Fig. 2,3) The patient was managed by stretching and warm massage under supervised care. A schedule of five days of therapy resulted in dramatic improvement in pain scores and morbidity.
RESULT
The pain profile as measured by 10 point visual analogue score (VAS) and 100 point numerical rating scale (NRS) was substantially improved with patient pain free and performing activities of daily living in follow up at 6 and 12 weeks and finally at 3 months.
CONCLUSION
The anticipation of DOMS and its early management can save agony and pain involved in delay of appropriate care. At times, advance imaging modalities like MRI can be instrumental in diagnosis as well as to rule out other sinister disorders.
DISCUSSION
Micro-structural tear within muscle and connective tissues, lactic acidosis, inflammation and spasm has been attributed to clinical symptoms of DOMS.[1] Often peaking 1-3 days after unaccustomed physical exertion, the exact etiology of disease is unclear with only few hypotheses described. Structural damage to contractile tissue, disruption of calcium homeostasis and certain chemical products accumulation in interstitium stimulating free nerve endings is one such proposed mechanism in the previous work. [2] The role of inflammatory mediators in the causation of the disease is also an area of concern. [3] Quadriceps, hamstrings and triceps surae are commonly involved muscle groups. It may be considered sign of regenerative process helping build stronger muscular tissues.[4] There is no universal guidelines to treat DOMS owing to multiple treatment modalities each with inconsistent efficacy.[5] Warm up, stretching and massage has been widely used physical treatment modalities with good outcome to treat DOMS.[6]
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Conflict of interest – None.
Source of funding – None
References:
1. Cheung K, Hume P, Maxwell L. Delayed onset muscle soreness: treatment strategies and performance factors. Sports Med. 2003;33(2):145-64.
2. Armstrong RB. Mechanisms of exercise-induced delayed onset muscular soreness: a brief review. Med Sci Sports Exerc.1984;16(6):529-38.
3. MacIntyre DL, Reid WD, McKenzie DC. Delayed muscle soreness.The inflammatory response to muscle injury and its clinical implications.Sports Med. 1995;20(1):24-40.
4. Coudreuse JM, Dupont P, Nicol C. Delayed post effort muscle soreness. Ann Readapt Med Phys. 2004;47(6):290-8.
5. Connolly D.A.J. ,Sayers S.P., Mchugh M.P. Treatment and Prevention of Delayed Onset Muscle Soreness. Journal of Strength and Conditioning Research, 2003, 17(1), 197– 208.
6. Rodenburg, J.B., Steenbeck D, Schierect P, Bar PR. Warmup, stretching and massage diminish harmful effects of eccentric exercise. Int. J. Sports Med. 15:414–419. 1994.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





