IJCRR - 7(1), January, 2015
Pages: 34-38
Print Article
Download XML Download PDF
PROSPECTIVE STUDY OF VAGINAL DISCHARGE AND PREVALENCE OF VULVOVAGINAL CANDIDIASIS IN A TERTIARY CARE HOSPITAL
Author: Twinkle N. Gandhi, Manish G. Patel, Mannu R. Jain
Category: Healthcare
Abstract:Objective: To study the etiology of vaginal discharge and to detect prevalence of Candida in patients with vaginal discharge from patients attending at SMIMER medical college, Surat, Gujarat.
Material & Methods: The present study was carried out in the Department of Microbiology, SMIMER medical college, Surat during the period of July 2010 to October 2011. A total 410 suspected cases of vaginal discharge, attending Obstetrics & Gynaecology OPD were included in the study. Detailed history of all patients was taken. All women were subjected to gynecological examination, pH test and Whiff test. Two swabs were collected one for direct microscopy and one for culture and sent immediately to the laboratory for microbiological examination.
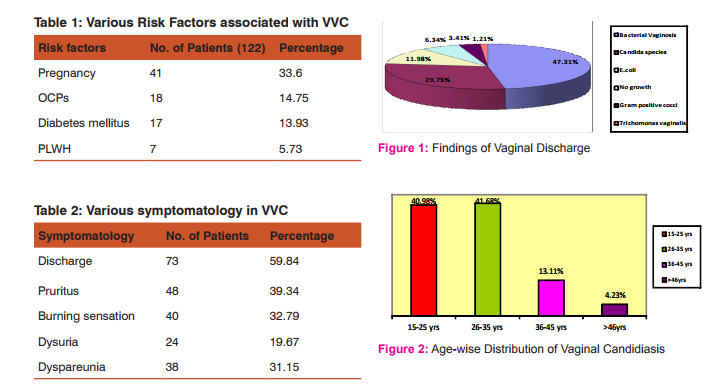
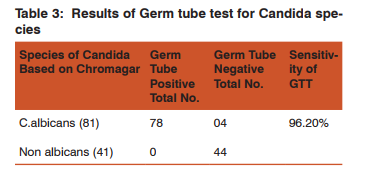
Results: The percentage of Bacterial vaginosis was the highest (47.31%) followed by Candida species (29.75%), E.coli (11.98%), Gram positive cocci (3.41%) and least was Trichomonas vaginalis (1.21%). The age group which was most prone to the infection was 26-35years (41.68%), followed by 15-25 years (40.98%), 36-45 years (13.11%) and least in >46 years (4.23%). Among VVC various associated risk factors observed, like pregnancy (33.6%), OCPS (14.75%), Diabetes mellitus (13.93%) and HIV (5.73%). Conclusions: In our study the most common pathogen in vaginal infections was Bacterial vaginosis (47.31%) followed by Candida species (29.75%). Distribution of Candida species among different age groups showed the highest incidence in reproductive age group of 26 \? 35 years, followed by 16 \? 25 years. VVC is more common with risk factors like pregnancy and Diabetes mellitus.
Keywords: RTIs, Bacterial vaginosis, VVC, Candida Spp., Vaginal discharge
Full Text:
INTRODUCTION
Vaginitis is the commonest Reproductive tract infections (RTIs) in sexually active females.2, 12 RTIs are the major public health problems among women especially in developing countries.2 WHO estimates that approximately 340 million new cases of curable STIs (Sexually transmitted infections) occur every year and majority of them from developing countries.12,15 Vaginitis is usually characterized by a vaginal discharge and/ or vulvar itching and irritation.4 The three diseases most frequently associated with vaginal discharge are Bacterial Vaginosis (replacement of the normal vaginal flora by an overgrowth of anaerobic microorganisms, myco-plasmas, and Gardnerella vaginalis), Trichomoniasis (T.vaginalis) and Candidiasis (usually caused by Candida albicans).15,4 Even in the modern advances in medicine, there is a rise in the incidence of fungal infections especially those due to Candida species.1 Vulvovaginal candidiasis (VVC) affects up to 75% of reproductive-age women at least once, nearly half will experience recurrences, and 5%–8% have multiple episodes each year.VVC is diagnosed in up to 40% of females with vaginal complaints. 4 ,22Candida species are the normal microbial flora within the gastrointestinal tracts, respiratory tracts, vagina and the mouth.23Under certain conditions, such as prolonged antibiotics therapy, use of contraceptives, malnutrition, pregnancy, diabetes, obesity, tissue transplant, use of immunosuppressant drugs, neutropenia Candida may become pathogenic and cause candidiasis. The majority of these infections are caused by Candida albicans. 3
Diabetes mellitus predisposes individuals to bacterial and fungal infections. Chronic recurring VVC may be a marker of diabetes.18 It is reported that the increase in occurrence of VVC during pregnancy is due to increased levels of hormones such as estrogen and steroid hormones.4,8 If the disease is not treated the baby can get infected (oral thrush) at birth which can be a serious health problem in premature babies.5,19,21 Untreated vaginal infections can lead to pelvic inflammatory disease and infertility.5,19 Sexual intercourse with an infected person is the most common mode of spread of genital candidiasis.12 Clinical diagnosis is based on signs, symptoms and confirmation done by laboratory diagnosis. Vulvar pruritus with vaginal discharge are the dominant feature of vulvovaginal candidiasis.8 The discharge is classically described as thick, adherent, and “cottage cheese-like” with a pH of 4.0 - 4.5.1, 20 To diagnose bacterial vaginosis, Amsel’s criteria is used worldwide. The criteria includes: (i) pH above 4.5; (ii) fishy odour with or without addition of 10 % KOH (Whiff test); (iii) homogenous, milky or creamy vaginal discharge; and (iv) presence of clue cells on microscopic examination. Presence of three out of four criteria is necessary for diagnosis of BV.7, 9 Another criteria for diagnosis of BV is Nugent’s score.6, 17 The prevalence of T.vaginalis ranges from 0.4–27.4% in women. The characteristic frothy, purulent discharge, punctate haemorrhagic areas called “strawberry cervix”, lower abdominal pain and dyspareunia seen in infection with T.vaginalis. 11 Many studies have reported the incidence of specific and non-specific organisms in their population. Gram Positive cocci (group B streptococcus) is a common organism to colonize the vagina. Enterobacteriacea group of organisms are also isolated from culture of vaginal discharge in laboratory. 24
MATERIAL & METHODS
The present study was carried out in the Department of Microbiology, SMIMER medical college, Surat during the period of July 2010 to October 2011 (15/7/2010 to 15/10/2011). A total 410 patients of suspected cases of vaginal discharge, attending Obstetrics &Gynaecology OPD were included in the study. A detailed history was taken with particular reference to name, age, and address, OPD no., presence of predisposing factors, onset and duration of complaints, treatment taken. All patients were asked about a standard questionnaire on their symptoms (vaginal discharge, vulvovaginal itching, vulvovaginal burning sensation, dysuria and dyspareunia). The amount, colour, character and smell of vaginal discharge were noted. Two sterile swabs were used for collection of discharge from lateral and posterior vaginal walls: (i) First swab was used for Amine test, wet mount examination and for gram’s staining. (ii) Second was used for culture on Sabouraud’s dextrose agar, Blood agar and MacConkey’s agar.
Laboratory procedures done:
a) Amine Test: A drop of 10% KOH was added to the vaginal secretions taken on a clean glass slide and fishy odour was noticed.
b) Wet mount examination: The vaginal secretions taken on a clean glass slide and a drop of normal saline added, mounted with a cover slip. No of pus cells and clue cells counted. Candida was identified as highly refractile, round or oval budding yeast cells.
c) Gram’s staining: Smears were prepared by the specimen and was fixed by flaming. Then the slide was stained by Gram’s Method and was examined under microscope for detection of gram positive budding yeast cells with or without pseudohyphae and any bacterial organisms.
d) Culture: Culture was done on Blood agar, MacConkey’s agar and Sabouraud’s dextrose agar. Incubated at 37?C for 24 and 48 hours and colony morphology observed.
e) Final Identification: In case of Candida the species identification was done based on gram staining, germ tube test and inoculation on CHROM agar following standard methods. In case of bacterial pathogen identification was done based on colony morphology, gram stain and biochemical reaction.
RESULTS AND ANALYSIS
Among the 410 vaginal specimens collected from the patients attending Obstetrics & Gynaecology department 26 (6.34%) samples were negative for any pathogen. Among the positive samples the percentage of Bacterial vaginosis was highest (47.31%) followed by Candida species (29.75%), E.coli (11.98%), Gram positive cocci (3.41%) and least was Trichomonas vaginalis (1.21%) (Figure 1). The age of patients was between 19 to 55 years in our study. The prevalence of Candida species was found to be more in reproductive age group, maximum in the age group of 26 to 35 years (41.68%) and 15 to 25 years (40.98%) followed by 36 to 45 years (13.11%) and least in 46-55 years (4.23%) (Figure-2). Among 122 candidiasis case various associated risk factors like Pregnancy (33.60%, 41/122), OCP use (14.75%, 18/122), Diabetes mellitus (13.93%, 17/122) and PLWH (5.73%, 7/122) were observed (Table 1).
Among 122 patients with VVC various symptoms like vaginal discharge were seen in 59.84%(73/122), pruritus in 39.34% (48/122), burning sensation in 32.79%(40/122), dysuria in 19.67% (24/122) and dyspareunia in 31.15% (38/122)(Table 2). Out of total 122 Candida isolates 78 isolates were germ tube test positive and 44 isolates showed germ tube test negative. All yeast isolates were also inoculated on CHROM agar (We had considered CHROMagar as a gold standard method). CHROMagar had shown 81 C.albicans (66.39%) while 41 as non albicans spp. (33.60%) (Table 3).
DISCUSSION
Despite therapeutic advances, vulvovaginal Candidiasis remains a common problem worldwide, affecting all strata of society. Their epidemiological profile varies from country to country and from one region to another within a country depending upon demographic, Socioeconomic and health factors.12 In our study we have found no any pathogen in 6.34% of cases. In Thulkar et al 9 14.36% were of no growth. In our study we have found 11.98% of E.coli that is in correlation with 14% in Puri etal16, while 10% in Fauzia et al10. In our study prevalence of gram positive cocci is 3.41%, while it is 8% in Fauzia et al10. The incidence of bacterial vaginosis in our study (47.31%), while in Puri et al 16 31% and in Thulkar et al 9 39.01%. Among 410 symptomatic women studied, the prevalence of Candida species were 29.75%. The similar pattern of isolation was found in Puri et al16 31% while Fauzia et al 10 found 40%. The incidence of Trichomonas vaginalis in our study is 1.21%, which has good correlation with Puri et al16(2%). The present study was carried out to isolate and characterize the Candida spp. from vaginal discharge of reproductive age. Maximum incidence of VVC in our study was in 26-35 yr. age group 41.68%, other studies showed little higher rate of candidiasis Okungbowa FI et al 8 56.00% and Babin et al2749.58%. VVC is more likely to occur in pregnancy. In our study we found 33.6% patients with pregnancy while similar data in L.B et al25and in Nwadioha et al26 are 44.8% & 40%, respectively. Diabetes mellitus is also another important risk factor in VVC. In present study, we observed 13.93% of VVC with D.M, whereas Nwadioha et al26 observed 7.14%. Other risk factors like HIV/AIDS and OCPs users in our study were 5.73% and 14.75%, respectively while data in Nwadioha et al2612.14% and 15% respectively. In present study Various symptoms of VVC like vaginal discharge(59.84%), pruritus(39.34%), burning sensation(32.79%), dysuria(19.67%) and dyspareunia(31.15%) were found which are in good correlation with Lopes ME et al28 study who found vaginal discharge(57.58%), pruritus(36.36%), burning sensation(45.45%), dysuria(24.24%) and dyspareunia(36.36%). Sensitivity of GTT in our study is 96.2% which is quite comparable with J.E. Hoppe et al13(98.9%) and Arthur E. Crist et al14(94.7%).
CONCLUSION
Proper diagnosis of cases of vaginal discharge is required to know the exact aetiological agent. Vaginal discharge, pruritus, burning sensation, dysuria and dyspareunia are the common complains. Such symptoms may occur due to candidiasis, non candidal pathogen and other factors. This study has shown that Bacterial vaginosis is the most predominant aetiology followed by Candida species. We concluded that discharge and pruritus were the most common symptoms of vulvovaginal candidiasis. Distribution of Candida species among different age groups showed the highest incidence in age group of 16 – 35 years. Candidiasis is more common in pregnancy and diabetic patients. Germ tube test will differentiate between albicans and non-albicans species of Candida. CHROMagar is an easy and reliable method for the identification of various species of Candida.
ACKNOWLEDGEMENT
Authors would like to thank Dean and Medical Superintendent, SMIMER Medical College and hospital for allowing us to carry out this study and for providing the facilities and help. They are also thankful to the Head of Department Obstetrics & Gynecology, SMIMER Medical College and hospital for allowing us to collect the specimens of their patients. Authors would also like to extend their gratitude to authors whose articles are cited and included in the references of the present study. They are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. E. E. Akortha, V. O. Nwaugo and N. O. Chikwe. Antifungal reistance among Candida species from patients with genitourinary tract infection isolated in benincity,Nigeria. African Journal of Microbiology Research Vol.3 (11) pp.694- 699; November 2009.
2. Sangeetha S Balamurugan, ND Bendigeri.CommunityBased Study of Reproductive Tract Infections Among Women of the Reproductive Age Group in the Urban Health Training Centre Area in Hubli, Karnataka. Indian Journal of Community MedicineVol 37;Issue 1,January 2012.
3. MahnazMahmoudi Rad, AmenehSh Zafarghandi, Maryam Amel Zabihi,MahkamTavallaee, and Yasaman Mirdamadi. Identification of Candida Species Associated with Vulvovaginal Candidiasis byMultiplex PCR.Infectious Diseases in Obstetrics and GynecologyVolume 2012, Article ID 872169.
4. R. Scott McClelland, Barbra A. Richardson, Wisal M. Hassan,Susan M. Graham, James Kiarie, Jared M. Baeten et al. Prospective Study of Vaginal Bacterial Flora andOther Risk Factors for Vulvovaginal Candidiasis;Vaginal Bacterial Flora and VVC.The Journal of Infectious Diseases 2009; 199:1883–90.
5. P. Madhivanan ,K Krupp,VChandrasekaran, C Karat, A Arun, CR Cohen et al. Prevalence and corelates of bacterial vaginosis among young women of reproductive age in mysore. Indian journal of medical microbiology (2008)26(2):132- 7.
6. Indulata ,Yashodhara Pradeep, Sujata, Amita Jain. Estimation of the incidence of bacterial vaginosis and other vaginal infections and its consequences on maternal/fetal outcome in pregnant women attending an antenatal clinic in a tertiary care hospital in north india.Indian Journal of Community Medicine,Vol 35;Issue 2,April 2010.
7. Centers for Disease Control and Prevention; Sexually Transmitted Diseases guidelines; 2006.
8. Francisca I. Okungbowa, Omoanghe S.Isikhuemhen & Alice P. O. Dede.The distribution frequency of Candida species in the genitourinary tract among symptomatic individuals in Nigerian cities. Rev Iberoam Micol 2003; 20: 60-63.
9. JyotiThulkar, AlkaKriplani&Nutan Agarwal.Utility of pH test & Whiff test in syndromic approach of abnormal vaginal discharge. Indian J Med Res 131;March 2010, pp 445- 448.
10. Fouzia Khan, RakhshandaBaqai. In vitro antifungal sensitivity of fluconazole, clotrimazole and nystatin against vaginal candidiasis in females of childbearing age. J Ayub Med Coll Abbottabad 2010;22(4).
11. Seema Sood, Arti Kapil. An update on Trichomonas vaginalis.Indian J Sex Transm Dis 2008; Vol. 29, No. 1.
12. Arul Sheeba, Malar S., Viswanathan T., Malarvizhi A., Lavanya V. and Moorthy K. Isolation, characterisation and antifungal susceptibility pattern of Candida albicans and non albicans Candida from Integrated counselling and testing centre (ICTC) patients.African Journal of Microbiology Research ;Vol. 6(31), pp. 6039-6048, 16 August, 2012.
13. J.E. Hoppe, P. Frey.Evaluation of Six Commercial Tests and the Germ-Tube Test for Presumptive Identification of Candida albicans. Eur J ClinMicrobiol Infect Dis (1999) 18:188–191.
14. Arthur E. Crist, Theresa J. Dietz, And Kristin Kampschroer. Comparison of the MUREX C. albicans, Albicans-Sure, and BactiCard Candida Test Kits with the Germ Tube Test for Presumptive Identification of Candida albicans. Journal Of Clinical Microbiology, Oct. 1996, p. 2616–2618, Vol. 34, No.10.
15. William J. Watson, Gregory DeMarchi : Vaginal Discharge: An approach to diagnosis and management Can. Fam. Physician Vol. 33: August 1987.
16. Puri KJ, Madan A, Bajaj K.Incidence of various causes of vaginal discharge among sexually active females in age group 20-40 years. Indian Journal Of Dermatology,Venereology And Leprology;Year: 2003, Volume : 69 , Issue : 2 ,Page : 122-125.
17. SrujanaMohanty, SeemaSood, ArtiKapil&Suneeta Mittal. Interobserver variation in the interpretation of Nugent scoring method for diagnosis of bacterial vaginosis. Indian J Med Res. 131, Januray 2010, pp 88-91.
18. Ella M de Leon, Scott J Jacober, Jack D Sobel and Betsy Foxman. Prevalence and risk factors for vaginal Candida colonization in women with type 1 and type 2 diabetes 1. BMC Infectious Diseases 2002.
19. Oviasogie F.E, and Okungbowa F.I. Candida species amongst pregnant women in benin City, nigeria: effect of predisposing factors. African journal of clinical and experimental microbiology;May2009 ISBN 1595-689x;vol 10(2).
20. Md. Abdullah Yusuf, Md. AbulQuashem Chowdhury,AbuNaser IbneSattar, Md. Mostaqimur Rahman. Evaluation of the Effect of Contraceptives on Prevalence of Candida Species on Vaginal Candidiasis in Dhaka, Bangladesh. Bangladesh J Med Microbiology 2007; 01 (02): 61-64.
21. Jack D Sobel.Vulvovaginal candidosis. Lancet 2007; 369: 1961–71Vol 369 June 9, 2007.
22. Flavia De Bernardis, Haiqun Liu, Rachel OMahony, Roberto La Valle, Silvia Bartollino, Silvia Sandini, et al.Human Domain Antibodies against VirulenceTraits of Candida albicans Inhibit Fungus Adherence to Vaginal Epithelium and Protect against Experimental Vaginal Candidiasis. The Journal of Infectious Diseases 2007; 195:149–57.
23. Jagdish Chander.Textbook of Medical Mycology.3 rded. New Delhi: Mehta publishers;May 2011.
24. Ismaeel Khan, Umar Ali Khan. A hospital based study of frequency of aerobic pathogens in vaginal infections Shifa College of Medicine, Islamabad, January 6, 2004.
25. Luciana Basili Dias, Marcia de Souza CarvalhoMelhem, Maria WalderezSzeszs,JoseMeirellesFilho, Rosane Christine Hahn. Vulvovaginal candidiasis in matograsso, Brazil: Pregnancy status,causative species and drug tests. Brazilian journal of Microbiology (2011) 42:1300-1307.
26. S. I. Nwadioha, D. Z. Egah, O. O. Alao. Risk factors for vaginal candidiasis among women attending primary health care centers of Jos, Nigeria. Journal of Clinical Medicine and Research Vol. 2(7), pp. 110-113, July 2010.
27. Deepa Babin,Subbannayya Kotigadde,P.Sunil Rao. Clinicomycological profile of vaginal candidiasis in a tertiary care hospital in Kerala.Inter. Journal of Research in Biological Sciences 2013; 3(1): 55-59.
28. Marcia Edilaine Lopes Consolaro, Thamara AlineAlbertoni, Celina Shizue Yoshida, JosmarMazucheli&Terezinha Inez EstivaletSvidzinski. Correlation of Candida species and symptoms among patients with vulvovaginal candidiasis in Maringa,Parana, Brazil. Rev IberoamMicol 2004; 21: 202- 205.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





