IJCRR - 7(3), February, 2015
Pages: 36-38
Print Article
Download XML Download PDF
RETINAL AND MACULAR HEMORRHAGES IN PLASMODIUM VIVAX INFECTION: AN UNCOMMON COMPLICATION
Author: Rajalakshmi A. R., Srikanth K., Maithreyee V.
Category: Healthcare
Abstract:Aim: To study the association between retinal hemorrhages in Plasmodium vivax malaria infection.
Case report: A 29 - year -old male patient with fever and hepatosplenomegaly, diagnosed with Plasmodium vivax (P. vivax) malaria
infection developed sudden loss of vision in left eye during the course of illness. He was found to have retinal and macular
intra-retinal hemorrhage and was managed conservatively with serial follow up. The condition resolved spontaneously with no
residual defective vision.
Discussion: Retinal and macular hemorrhages are very rare in P. vivax infections and very few cases have been reported in
literature.
Conclusion: Recognition of this rare, yet serious and vision threatening complication in P. vivax malaria infection is emphasized
for the need to be aware of the protean manifestations of P. vivax malaria infections.
Keywords: Retinal hemorrhage, Macular hemorrhage, P. vivax
Full Text:
INTRODUCTION
Malaria is an infective disease caused by protozoa of Plasmodium species- vivax, falciparum, ovale and malariae. Malarial retinopathy consists of retinal whitening, retinal hemorrhages, and papilledema. [1] In P. vivax malaria, retinal hemorrhages are very rare and only nine cases have been reported so far. [2-6,8,9] We herein describe a 29- year- old male with P. vivax infection who developed retinal and macular hemorrhages. This case is being reported for its rarity and the need to be aware of the protean manifestations in P. vivax malaria.
CASE REPORT
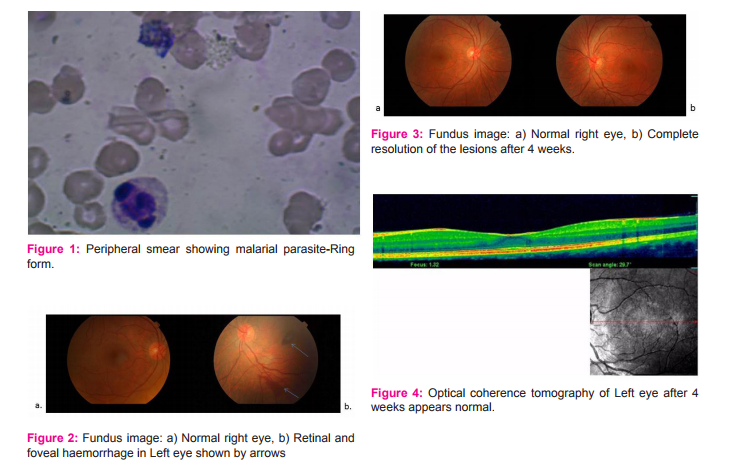
A 29 year old male was brought with complaints of high grade fever with chills for 5 days. On the fourth day of illness he had developed yellowish discoloration of the sclera; however the urine colour was normal. There was no history of altered sensorium, seizures, oliguria or bleeding manifestations. His relatives noted that he had become extremely pale during the period. On examination, he had severe pallor and icterus but no organomegaly. Soon after admission he developed hypotension and was shifted to the intensive care unit. Investigations were as follows: Hemoglobin was 4.1 g/dl, Total leucocyte count 18,500/mm3 , while platelet count was 54,000/mm3 . Serum bilirubin was 11mg/dl (indirect bilirubin 10.2 mg/ dl) with normal liver enzymes. Prothrombin time was normal. Blood urea was 95mg/dl while serum creatinine was 2 g/dl. Blood glucose and venous blood gas were normal. Peripheral blood smear was positive for Plasmodium vivax -ring form (Figure 1). He was managed in the intensive care unit with inotropes (dopamine and adrenaline) and packed red blood cell transfusions (twice). He never developed altered sensorium, oliguria or seizures. Artesunate combination therapy (intravenous artesunate with doxycycline) was administered for seven days in view of severe malaria followed by primaquine for 14 days. During the third day of intensive care unit stay, he developed ocular symptoms in the form of sudden painless diminution of vision in his left eye. His ocular examination showed a Best Corrected Visual Acuity (BCVA) 20/20 in Right Eye (RE) and 20/120 in the Left Eye (LE). Anterior segment examination was normal in both the eyes. Fundus examination of the right eye was normal and in the left eye, showed an intra- retinal hemorrhage two disc diameter away from the disc along the inferior temporal arcade and a hemorrhage involving the fovea measuring about one disc diameter (Figure 2). The patient was managed conservatively and kept under serial observation. He was shifted out of the intensive care unit on the sixth day of admission. Icterus resolved and fever subsided. Blood urea and serum creatinine normalized at discharge after 10 days. At discharge, the intra-retinal hemorrhage along the infero-temporal arcade was slightly smaller and resolving while the hemorrhage at the fovea remained the same with visual acuity of 20/120 in left eye and right eye was normal. On follow up after four weeks, there was complete resolution of the hemorrhage in the left eye and visual acuity was 20/20 (Figure 3). Optical coherence tomography at follow up was done which showed a normal retina and no residual changes (Figure 4).
DISCUSSION
Malaria is a highly prevalent disease caused by various species of Plasmodium. P. vivax and P. falciparum are the common pathogens in our part of the world with P. vivax being more common in south India. [7] Ocular complications in malaria have been reported in 10% to 20% of patients. [10] Ocular manifestations are more with P. falciparum than with other types. The severity of malarial retinopathy correlates with the mortality associated with malaria. [1] The retina is embryologically a part of the central nervous system and shares a common cellular structure and blood retina barrier which predisposes the retina and neurological structures to complications of malaria. Ocular manifestations of malarial retinopathy include retinal whitening, vessel discoloration, retinal hemorrhages and papilloedema. Retinal hemorrhages can be intra retinal white centered, similar to Roth’s spots, flame shaped and also large blot hemorrhages. Reduced blood flow and cyto-adherent erythrocytes sequestrated in microvasculature with resultant non-perfusion are hypothesized to be the cause for these retinal changes. [1] Thrombocytopenia and anaemia, as observed in our patient, also may contribute to intra-retinal hemorrhage. There is a paucity of cases of P.vivax in association with intra-retinal hemorrhages. Overall very few anecdotal reports of cases of retinal hemorrhages in P. vivax malaria have been reported so far in the literature[2-6,8,9] of which five were from India and rest four from South Korea. All the reported cases had retinal hemorrhages and six also had sub- hyaloid hemorrhage in addition. Cotton wool spot was reported in only one of the cases. In all these cases there was spontaneous resolution of the hemorrhages in 1-6 weeks and good functional recovery of vision. However 2 cases had foveal hemorrhage which lasted longer than other lesions and these patients had a decrease in visual acuity and hemotoxicity to photoreceptors was considered as a possible cause. A notable feature of our patient was that he had retinal as well as foveal haemorrhage. Inspite of this, there was complete resolution of the lesions with complete morphological and functional recovery. This case is being reported for its rarity and also to be aware of the retinal complications of P. vivax malaria by the treating physicians, since they contribute to significant morbidity. There have been only anecdotal reports of retinal hemorrhages in P. vivax malaria. Hence this ocular complication is not well recognised among Ophthalmologists. Through this report we wish to emphasise that there is a need to be aware of complications such as retinal hemorrhages even in malaria due to “seemingly benign” Plasmodium species such as P. vivax. In fact the term “benign tertiary malaria”, classically caused by P. vivax is increasingly considered a misnomer due to such serious complications associated with the condition.
CONCLUSION
The authors emphasize that although retinal manifestations are exceedingly rare in P. vivax infections, recognition of such complications would help in further delineation and expansion of the varied clinical presentations of P. vivax malaria.
ACKNOWLEDGEMENTS
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Sithole HL. A review of malarial retinopathy in severe malaria. S Afr Optom 2011; 70:129-35.
2. Biswas J, Fogla R , Srinivasan P , Narayan S , Haranath K , Badrinath V . Ocular malaria. A clinical and histopathologic study. Ophthalmology 1996; 103: 1471-5.
3. Kim SM, Kim KB, Jung HJ, Kim WJ, Kim MJ, Park SC. Retinal hemorrhage in an adult with P. vivax malaria. Korean J Infect Dis 1997; 29: 323-6.
4. Chung C, Kim Y, Chung M. Retinal hemorrhage in a patient with tertian malaria. Korean J Infect Dis 1998; 30: 115.
5. Choi HJ, Lee SY, Yang H, Bang JK. Retinal haemorrhage in vivax malaria. Trans R Soc Trop Med Hyg 2004; 98: 387-9.
6. Lee JH, Chin HS, Chung MH, Moon YS Retinal hemorrhage in Plasmodium vivax malaria. Am J Trop Med Hyg. 2010; 82: 219-22.
7. Kumar A, Valecha N, Jain T, Dash AP. Burden of Malaria in India: Retrospective and Prospective View. In: Breman JG, Alilio MS, White NJ, editors. Defining and Defeating the Intolerable Burden of Malaria III: Progress and Perspectives: Supplement to Volume 77(6) of American Journal of Tropical Medicine and Hygiene. Northbrook (IL): American Society of Tropical Medicine and Hygiene; 2007 Dec. Available from: http://www.ncbi.nlm.nih.gov/books/NBK1720/
8. Sharma S, Maheshwari U, Bansal N. Retinal haemorrhage in plasmodium vivax patients-2 rare case reports. J Evolution Med Dent Sci .2012:1;929-31
9. Kochar A, Kalra P, Kochar S, Kochar SK, Kochar D. K. Retinal haemorrhage: An unusual presentation of vivax malaria. J Vector Borne Dis: 2013: 50; 321-322.
10. Hidayat AA, Nalbandian RM, Sammons DW, Fleischman JA, Johnson TE. The diagnostic histopathologic features of ocular malaria. Ophthalmology.1993; 100:1183-6.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





