IJCRR - 7(3), February, 2015
Pages: 01-07
Print Article
Download XML Download PDF
EFFICACY OF NARROW BAND VERSUS BROAD BAND IN TREATMENT OF PITYRIASIS ROSEA
Author: Intsar S. Waked, Abdel Hamid N. Deghidi
Category: Healthcare
Abstract:Background: UV phototherapy has recently demonstrated high levels of efficacy and tolerability for treating a variety of inflammatory skin diseases. Objective: The purpose of the present study was to evaluate the efficacy of narrow band versus broad band in the treatment of pityriasis rosea. Methods: Twenty patients (12 female & 8 male) with extensive pityriasis rosea type III & IV were participated in the study. Their ages ranged between 18 and 35 years.The right half of the body of each patient was irradiated with NB-UVB ,while left side of each patient is exposed to broadband BB-UVB for 3 times alternatively per week until clearing of lesions or for 6 weeks. The rate of clearing was monitored by estimating the pityriasis rosea severity (PRSS) score and the pruritus score. Results: The extent of disease (PRSS) for Rt side decreased from (34.30\?10.16vs. 10.50\?7.00, respectively< 0.05) while for Lt side (35.90\?10.31.vs. 16.00\?9.06). The percentage of reduction in intensity of puritis were 53%, 49%, for NBUVB side and BBUVB side respectively. Conclusion: This study shows that NBUVB was more effective than BBUVB in reduction of PRSS and the degree of pruritus in pityriasis rosea.
Keywords: Pityriasis rosea, Pityriasis rosea severity score, UVNB and UVBB
Full Text:
INTRODUCTION
Pityriasis rosea (PR) is a skin disorder that describes a sudden appearance of discrete plaques (patches) of skin rash in a distinctive pattern over the body and limbs. ’Pityriasis’ (meaning bran-like), indicates that there are scales in the skin lesions. ‘Rosea’ means rose-like and describes the typical colour of the rash, although the colour varies to a wide extent in different races. [1] Pityriasis rosea (also known as pityriasis rosea Gibert) is a skin rash. It is benign but may inflict substantial discomfort in certain cases. Classically, it begins with a single “herald patch” lesion, followed in 1 or 2 weeks by a generalized body rash lasting up to 12 weeks [2-5] Pityriasis rosea (PR) is an acute, self-limited papulosquamous disorder that begins with the appearance of an initial plaque most often on the trunk, and this is followed in about a week or two by the development of an analogous spotty rash and it usually persists for 4~7 weeks. The exact etiology of the disease is still unknown, although active infection with both human herpes viruses 6 and 7 is thought to play a role in PR.[6] Pityriasis rosea is a harmless skin disease that causes scaly patches that sometimes itch over the torso, neck, arms and legs. Anyone can get it, but it is most common in people ages 10 to 35. About 50% of all people with PR have itching of moderate to severe intensity. The quality of life of people with PR is significantly affected. Parents of children with PR also have significant anxieties about the cause, nature, and possible infectivity of the eruption.[7, 8] No specific therapy is available and in many cases none is needed; however, some patients have an extensive eruption and considerable pruritus. For patients with severe pruritus, experts have recommended treatment with zinc oxide, calamine lotion, topical steroids, oral antihistamines and even oral steroids. Ultraviolet radiation, through artificial sources or intentional exposure to natural sunlight, has been recommended to decrease the duration of the rash and the intensity of itching in patients with pityriasis rosea [9,10] The American Academy of Dermatology defines phototherapy as the exposure to nonionizing radiation for therapeutic benefit. It may involve exposure to ultraviolet (UV)A, UVB, or various combinations. Phototherapy can be administered in inpatient hospital settings, hospital clinics, daycare centers, and doctor’s offices, as well as for home therapy. Many diseases have been reported to respond to this treatment, including psoriasis, hand dermatitis, mycosis fungoides, pruritus, pityriasis rosea, lichen planus, pityriasis lichenoides, and many more. [11-14] Phototherapy with ultraviolet (UV) radiation of wavelengths between 280 and 320 nm (UVB) is a safe and effective treatment for a variety of diseases. There are two types of UVB treatment, broadband (bUVB) and narrowband (nUVB) (TL /01). Phototherapy with bUVB or nUVB has been reported to be effective and safe for the treatment of a large number of skin diseases. Narrowband UVB is similar to broad-band UVB in many ways. The major difference between them is that narrowband UVB is light energy which is emitted in a narrow portion of the UVB range which is concentrated in the therapeutic range, with an optimum peak at 311 nm.[15-19] The aim of this study was to evaluate the efficacy of narrow band versus broad band in the treatment of pityriasis rosea.
Patients & Methods
Twenty patients ( 12 female & 8 male ) with extensive pityriasis rosea were participated in the study. Their ages ranged between 18 and 35 years and had skin type III & IV. Diagnosis of pityriasis rosea was made by two dermatologists for all patients, based on characteristic clinical features. Signed informed consent was obtained from each patient before enrollment in the study. Reasons of exclusion are pregnant women, patients had history of photosensitivity, skin malignancy, abnormal reactions to sunlight or immunosuppression, patients were taking potentially phototoxic or immunosuppressive medication. Also if either of the dermatologists did not agree with the diagnosis of pityriasis rosea, the patient was not eligible for enrollment. and those with the absence of pruritus at the time of diagnosis were excluded from the study. Standardized case record forms were used for the purpose of collecting basic characteristics of the patients, which included age, sex, duration of rash, the season during presentation, history of preceding upper respiratory infection, exposure to a patient of pityriasis rosea, and herald patch. Complete blood counts and antistreptolysin-O titers were carried out in all patients and venereal disease research laboratory (VDRL) test was performed to exclude secondary syphilis. The experimental protocol was explained in details for each patient before the initial assessment.
Measurement Methods
The severity of the disease was determined according to the Pityriasis Rosea Severity Score (PRSS). Intensity of pruritus was determined by visual analogue scale (VAS).
Measurement the severity of pityriasis rosea [20]
Two areas were assessed for determining the PRSS (1) the head and trunk (t) and (2) the upper and lower extremities (e). The extent of the disease was first assessed with a 0 to 3 scale (0=absence of lesions, 1=1 to 9 lesions, 2=10 to 19 lesions, 3=≥20 lesions). To evaluate the severity of the lesions, three target symptoms termed erythema (E), infiltration (I) and scale (S) were assessed according to a scale of 0 to 3, in which 0 means a complete lack of cutaneous involvement and 3 represents the most severe possible involvement. To calculate the PRSS, the sum of the severity rating for these three main changes was multiplied with the numeric value (N) of the extent of the disease. The formula can be written as: PRSS=Nt (Et+It+St)+Ne (Ee+Ie+Se). The subscript “t” indicates one side of the trunk and the head, and the subscript “e” indicates one side of the extremities. Improvement in PRSS was graded as the percentage reduction as follows: minimal, ≤25%; good, 26-50%; very good, 51-75% and >75%, was excellent. A patient’s condition was defined as clearing if he or she had a PRSS score of 2 or less Assessment the pruritus a 100-mm visual analog scale was used to assess the severity of pruritus pre and post treatment. This scale has been extensively used and demonstrated to be a valid instrument for the measurement of intensity of pruritus . A horizontal line made on a sheet of paper with the left end marked as no symptoms and the right end marked as worst imaginable symptoms. The patient was asked to draw a vertical line to indicate the intensity of the symptom. The length from the left end to the vertical mark made by the patient was measured in millimeters.[21]
Treatment Procedures
Determination of the initial dose: Before initiating phototherapy, the initial irradiation dose for the individual patient must be determined. The dosage of UV light is prescribed according to an individual’s skin sensitivity. Thus, to establish the proper dosage of UV light to administer to a patient, the patient is screened to determine a minimal erythema dose (MED).The patient’s MED is determined by exposing six small template areas (eg, circles of 1 cm diameter) of nonexposed skin (lower back, buttocks) to an incremental series of UVB irradiations. Increases are made by fixed values (eg, 10 mJ/cm2). The MED is defined as the lowest dose that causes a minimally perceptible erythema reaction 24 hours after irradiation. Sunbathing or exposure to solaria must be avoided before phototesting. The type of lamp used for MED determination should be documented, since values obtained with broadband or narrowband sources are markedly different.
Treatment protocol
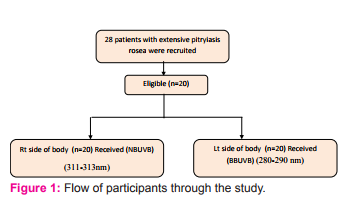
The right half of the body of each patient was irradiated with NB-UVB (311-313nm) with the average peak at 313 nm. by Philips UVB Narrowband TL100W/01 with output 17.7 w, Lamp voltage is 126, Lamp current 0.97 and with cap base R17d. The left side of each patient is exposed to broadband ultraviolet B 290-325nm (BB-UVB) by Philips UVB Broadband TL100W/12 with output 12.7 w, Lamp voltage is 126, Lamp current 0.97 The initial treatment dose was 70% of the MED and the dose was increased by 10% if no erythema or discomfort developed from the prior irradiation, 5% with minor erythema not lasting longer than 24 h, and no increments if the erythema lasted more than 24 h. Therapy was given 6 times weekly ( 3 times for Rt side & 3 times for Lt side alternatively ) until clearing of lesions or for 6 weeks. At the day of session ask patient to wear protective goggles, not put perfumes, deodorants, aftershave lotions or other cosmetic products. Some of these contain additives which make the skin more sensitive to light as this may cause burn. The patients were asked not to expose themselves to ambient sunlight during the study. No other treatment had been given for at least 3 months prior to the start of study.
Statistical Analysis
Frequencies are used to describe the variables (Sex , skin type, occurrence of herald patch). Student t test was used to assess the difference between the studied parameters (PRSS, IP) between two sides of body while paired t test was used to analyze these parameters within each side pre and post treatment. Data were coded and entered to a statistical package of social science (SPSS, version 16). All P values less than 0.05 were considered to be statistically significant.
RESULTS
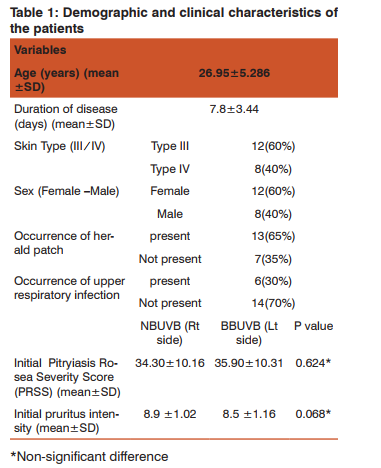
Figure 1, presents the flow chart for patients throughout the study. A total of 28 patients was screened for eligibility, and 20 subjects fulfilled the inclusion criteria and were completed the study and continued to the final analysis. Table 1 presents the demographic and clinical characteristics of the patients completing the study
Pitryiasis Rosea Severity Score Measurements (PRSS)
The severity of pitryiasis rosea disease was summarized in Table 2, as determined by Pitryiasis Rosea Severity Score (PRSS). The reductions in severity of disease were observed in NBUVB (Rt side) and BBUVB (Lt side) from initial (W0), to subsequent measurement at 6thweek (W6). Significant differences were found between two sides (10.50±7.00 versus 16.00±9.06, P<0.05) and percentage of reduction was 69%, 55%, for NBUVB side and BBUVB side respectively

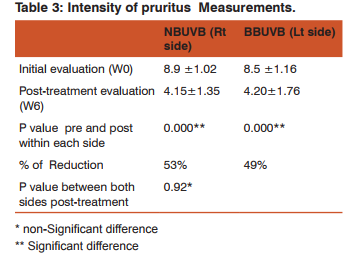
Intensity of pruritus Measurements (IP):
Intensity of pruritus was summarized in Table 3, as determined by Visual analogue Scale . The reductions in pruritus intensity were observed in NBUVB (Rt side) and BBUVB ( Lt side ) from initial (W0), to subsequent measurement at 6thweek (W6). No significant differences were found between two sides post treatment as P>0.05).
DISCUSSION
Today, phototherapy is a valuable option in the treatment of many non-psoriatic conditions including AD, sclerosing skin conditions such as morphea, vitiligo, and mycosis fungoides. Due to its relative safety, phototherapy may be used in most populations, including children and pregnant women. The UV range (10 to 400 nm) is further sub-divided into UVA and UVB, each of which has been particularly useful in a number of skin conditions. The most commonly used forms of UV irradiation are UVA1, PUVA, and NB-UVB, BBUVB. Each of these modalities differ in their mechanism of action, indications, and side effect profiles, and it is important that clinicians be familiar with these differences.[22] There have been a few reports of successfully treating pityriasis rosea using UV phototherapy, but there are currently no reports on comparing Narrow and broad band UVB in treating pityriasis rosea. [20] The purpose of this study to compare the efficacy of narrow band UVB versus broad band UVB in treating pitryiasis rosea. Twenty patients with extensive pityriasis rosea were participated in the study. The right half of the body of each patient was irradiated with NB-UVB (311-313nm) with the average peak at 313 nm. The left side of each patient is exposed to broadband ultraviolet B 290-325nm. Assessment was done through pitryiasis rosea severity score (PRSS) and visual analogue scale to assess severity of disease and pruritus. In our present study, out of 20 patients, 8 cases ( 40 % ) were males and 12 cases ( 60 % ) were female giving rise to male to female ratio of 1:1.5. This result was in accordance with a large study of Chuang et al, [23] who reported that the sex ratio was 1.5 females to 1 male patient. Crissey found twice as many females than males [24] while Cohen reported that both sexes were affected equally.[25] In most of the series reported, females preponderate over male but not so greatly.[26] On the other hand, Bjornberg and Hellgren reported a slight male preponderance.[27] Sharma et al as well as Vijyeeta reported a slight male preponderance.[28,29] preponderance. In our study there was a slight female preponderance. As regard to the duration of illness before entering the study varied from few days to few weeks. In our study most of the cases reported within 1st week illness (55 %) and ( 45% ) of the cases reported within 2nd week of illness. Early reporting to hospital was due to the presence of pruritus and anxiety caused by generalized appearance of the lesions over the body surface. In most of cases presented to us it was the first episode of pitryiasis rosea before the treatment could be initiated. Only 3 had episode of recurrence. History of upper respiratory tract was present in only 2 cases of pitryiasis rosea (10%). Chuang et al reported that history of cutaneous and non-cutaneous infections prior to onset of pitryiasis rosea was present in 16% of their cases and he found no association of pitryiasis rosea with atopy and sebborrheic dermatitis while Vijyeeta [29] reported 70% of cases had upper respiratory tract. Presence of herald patch was reported in about 85% cases and most commonly seen on the trunk (40%). This was in accordance with Vijyeeta [29] who reported that about 82% of cases demonstrated herald patch. Dambalkar K et al and various other authors in different studies have reported the incidence of herald patch to be 40- 76%. [23,30,31] Although the etiology of pityriasis rosea is unclear, several indicate an infectious cause. First, outbreak of the condition occur in clusters, suggesting an infectious agent is circulating within a community. Second, recurrence of pityriasis rosea outside the acute phase is rare, suggesting that there is long- lasting immunity after the infection. Third, up to 69 percent of patients with pityriasis rosea have a prodromal illness before the herald patch appear. Finally, some patients with pityriasis rosea show an increase in B lymphocytes, a decrease in T lymphocytes, and an elevated sedimentation rate. [32,33] The histologic features of pityriasis rosea are non-specific. In epidermis, mild hyperkeratosis with focal parakeratosis, minimal acanthosis with variable spongiosis, and a moderate exocytosis of lymphocytes with a thinned granular layer is present. In the dermis, extravasated red blood cells are accompanied by a perivascular infiltrate of lymphocytes and eosinophils with occasional monocytes. Similar findings are demonstrating in the herald patch with a deeper infiltrate and more pronounced acanthosis. Dyskeratotic cells are present in 50% of cases.[34-36] The results of the study showed that there were significant reduction in PRSS & VAS post treatment in both sides from W0 to subsequent W6 for both Rt (NBUVB) and Lt (BBUVB) side and this suggest efficacy of ultraviolet B in treating pitryiasis rosea controlling pruritus whatever the type of band . Valkova in his bilateral comparison study between UVA and UVB phototherapy in treatment of pityriasis rosea confirmed that the UVA irradiation in the dose mentioned earlier had no effect on the course of the disease but significant clinical improvement according to PRSS with total clearing of the rash was observed after UVB phototherapy[37], which is correlating with our study. Our study correlated with Leenutaphonga et al who in his study used a bilateral comparison experimental demonstrated that 10 daily erythemogenic exposures of UVB resulted in substantially decreased severity of disease in comparison with the control side in 15 of 17 patients. The overall reduction of PRSS showed a significant differences, the UVB irradiation was superior to UVA irradiation.[20] The results of this study was in accordance with a previous bilateral comparison study by Amdt et al in which five consecutive erythemogenic UVB phototherapy exposures were administered to one half of the bodies of 20 patients. It was shown that the extent of disease and pruritus on the treated side decreased more than on the untreated side [38]. As regard to the type of UVB band, the results of our study showed that NBUVB was more effective than BBUVB in reduction of PRSS with percentage of improvement was 69%, 55% respectively while there was no significant differences between NBUVB & BBUVB in reduction the degree of pruritus with percentage of improvement 53%& 49% respectively. Gambichler et al, [39] stated that Because NB-UVB may have a wider indication spectrum, including AD, vitiligo, and early-stage CTCL, and appears to be equally effective or even more effective than broad-band UVB (BB-UVB), a switch from BB-UVB to NB-UVB seems to be justified. On the other hand Pugashetti and colleagues[40] noted that BB-UVB phototherapy has demonstrated effectiveness in the treatment of cutaneous disorders including psoriasis, AD, uremic pruritus and idiopathic pruritus. Also they high-lighted in their report, that there was a small but significant proportion of psoriasis and AD patients who do not tolerate NB-UVB but demonstrated an excellent clinical response to BB-UVB. They reported that it is critical for dermatologists to recognize the role of BB-UVB as a complement to NB-UVB phototherapy for patients who cannot tolerate or experience an inadequate therapeutic response from NB-UVB. Our study was in accordance with Weiming Hui and other [41] who reported in their study good patient compliance and fewer adverse reactions, safe, reliable, and worthy of clinical application after 6 or 7 times of NBUVB irradiation treatment of pityriasis rosea. Also Samson et al reported that Narrow-band UVB phototherapy was well-tolerated, with no serious adverse effects and concluded that NB-UVB may be considered as a viable therapeutic option in the treatment of vitiligo, pruritus, and other inflammatory dermatoses. Several studies reported the immunomodulatory effects of nUVB appear to be more pronounced than bUVB [42]. Multiple studies have shown the effectiveness of narrowband UVB treatment to be superior to that of conventional broadband UVB treatment.[43,44] As regard to incidence of side effects, no significant sideeffect were noted during the treatment course by both types of UVB band except for slight burning sensation, darkening of the skin and dryness of the skin.
CONCLUSION
On conclusion our study showed that NBUVB was more effective than BBUVB in reduction of PRSS and the degree of pruritus in pityriasis rosea.
References:
1. Rapini, Ronald P.; Bolognia, Jean L.; Jorizzo, Joseph L. (2007). Dermatology: 2-Volume Set. St. Louis: Mosby. ISBN 1-4160-2999-0.
2. Jump up «Pityriasis rosea». American Osteopathic College of Dermatology. Retrieved 26 Jan 2010.
3. Jump up^ Freedberg; et al (2003). Fitzpatrick›s Dermatology in General Medicine (6th ed.). McGraw-Hill. p. 445. ISBN 0-07-138076-0.
4. Jump up^ James, William; Berger, Timothy; Elston, Dirk (2005). Andrews› Diseases of the Skin: Clinical Dermatology (10th ed.). Saunders. pp. 208–9. ISBN 0-7216-2921-0.
5. Jump up, Habif, Thomas P (2004). Clinical Der- Jump up, Habif, Thomas P (2004). Clinical Dermatology: A Clinical Guide to Diagnosis and Therapy (4th ed.). Mosby. pp. 246–8. ISBN 0-323- 01319-8.
6. Wong WR, Tsai CY, Shih SR, Chan HL. Association of pityriasis rosea with human herpesvirus-6 and human herpesvirus-7 in Taipei. J Formos Med Assoc. 2001;100:478–483.
7. Chuh AAT, Chan HHL. The effect on quality of life in patients with pityriasis rosea is it associated with rash severity?. International Journal of Dermatology 2005;44: 372–7.
8. Chuh AAT. Quality of life in children with pityriasis rosea - a prospective case control study. Pediatric Dermatology 2003;20:474–8.
9. Baden HP, Provan J. Sunlight and pityriasis rosea. Arch Dermatol. 1977;113:377–378.
10. Plemmons JA. Pityriasis rosea: an old therapy revisited. Cutis. 1975;16:120–121. 11. Drake LA, Ceilley RI, Dorner W, et al. Guidelines of care for phototherapy and photochemotherapy. J Am Acad Dermatol 1994; 31:643–8.
12. Feldman SR, Clark A, Reboussin D, et al. An assessment of potential problems of home phototherapy treatment of psoriasis. Cutis 1996;58:71–3.
13. Sjovall P, Christensen OB. Treatment of chronic hand eczema with UV-B Handylux in the clinic and at home. Contact Dermatitis 1994;31:5–8.
14. Harold JM, Vonderheld EC. Home ultraviolet phototherapy of early mycosis fungoides: preliminary observations. J Am Acad Dermatol 1982;6:355– 62.
15. Mark B, Martin RO¨ CKEN and Frauke B; Phototherapy with Narrowband vs Broadband UVB: Acta Derm Venereol 2005; 85: 98–108. 16. Van Weelden H, Baart de la Faille H, Young E, van der Leun JC. A new development in UVB phototherapy of psoriasis. Brit. J. Dermatol. 1988;119:11-19
. 17. B.E. Johnson, C. Green, T. Lakshmipathi and J. Ferguson, “Ultraviolet Radiation Phototherapy for Psoriasis: The use of a new Narrowband UVB fluorescent lamp”, Light in biology and medicine, p. 173, Plenum Press, NY and London (1988).
18. Barbagallo J, Spann CT, Tutrone WD, Weinberg JM. Narrowband UVB phototherapy for the treatment of psoriasis: a review and update. Cutis. 2001;68:345-7. Review.
19. Berneburg M, Roecken M, Benedix F. Phototherapy with Narrowband vs broadband UVB. Acta. Derm. Venerol. 2005; 85: 98-108.
20. Leenutaphong V, Jiamton S. UVB phototherapy for pityriasis rosea: A bilateral comparison study. J Am Acad Dermatol 1995;33:996-9.
21. Intsar S. Waked, Narrow Band Versus Broad Band Ultraviolet B Radiation in the Treatment of Patients with Generalized Lichen Planus; Bull. Fac. Ph. Th. Cairo Univ., Vol. 17, No. (1) Jan. 2012; 69-79.
22. Walker D, Jacobe H. Phototherapy in the age of biologics. Semin Cutan Med Surg. 2011;30(4):190- 198.
23. Chuang T, Perry O, Ilstrup DM, Kurland LT. Recent upper respiratory tract infection and pityriasis rosea: A case – control study of 249 matched pairs. Br J Dermatol 1983; 108: 587-91.
24. Crissey JT. Ptrclinityriasis rosea. Pediatrclin North Am 1956;3:801-9.
25. Cohen EL. Pityriasis rosea. Br J Dermatol 1967;79:553-537.
26. Sterling J. Virus infections. In : Burn, T Breathnach S, Cox N, Griffiths C editor. Textbook of Dermatology, 7th ed. Blackwell science Co: Oxford: London, 2004. P79-83.
27. Bjornberg A, Hellgren I. Pityriasis rosea-A statistical, clinical & laboratory investigation of 826 patients& matched healthy control. Acta Derm Venerol 1962;42(50):1-68.
28. Sharma PK, Yadav TP, Gautam PK, N, Satyanarayana L. Erythromycin in pityriasis rosea: a double – blind, placebo-controlled clinical trial. J Am Acad Dermatol 2000;422:241-4.
29. Vijayeeta J, study of therapeutic effect on UVB phototherapy in treatment of pityriasis rosea, Doctoral Thesis, Rajiv Gandhi University; 2013.
30. Dambalkar K pityriasis rosea with unusual herald patch Ind J Dermatol Venereol Leprol; 1998; 64(4):185-6.
31. Hurley HJ, Roberts. Localized pityriasis rosea. Aust J Dermatol 1961;12:52-3.
32. Baden HP, Provan J. Sunlight and pityriasis rosea. Arch Dermatol. 1977;113:377–378.
33. Plemmons JA. Pityriasis rosea: an old therapy revisited. Cutis. 1975;16:120–121.
34. Bunch LW, Tilley JC. Pityriasis rosea. A histologic and serologic study. Arch Dermatol, 1961;84: 79- 86.
35. Okamoto H, Imamura S, Aoshima T, Komura J, Ofuji S. Dyskeratotic degeneration of epidermal cells in pityriasis rosea : light and electron microscopic studies. Br J Dermatol 198;107(2): 189– 94.
36. Pannizon R, Bloch PH. Histopathology of pityriasis rosea Gibert. Qualitative and quantitative light-microscopic study of 62 biopsies of 40 patients. Dermatologica,1982;165:551–8.
37. Valkova S, Trashlieva M, Christova P. UVB phototherapy for pityriasis rosea. J Eur Acad Dermatol Venerreol 2004;18(1):111–2.
38. Amdt KA, Paul BS, Srern RS, Parrish JA. Treatment of pityriasis rosea with UV radiation. Arch Dermatol. 1983;119(5):381–2.
39. Gambichler T, Breuckmann F, Boms S, et al. Narrowband UVB phototherapy in skin conditions beyond psoriasis. J Am Acad Dermatol. 2005;52(4):660–670.
40. Pugashetti R, Lim HW, Koo J. Broadband UVB revisited: Is the narrowband UVB fad limiting our therapeutic options? J Dermatolog Treat. 2010;21(6):326–330.
41. Weiming Hui, Yue-Liaokang Huang. UVB Phototherapy Clinical observation on 72 cases of pityriasis rosea [J]. Journal of Clinical Dermatology, 1998,6:377.
42. Samson Yashar S, Gielczyk R, Scherschun L, Lim HW. Narrow-band ultraviolet B treatment for vitiligo, pruritus, and inflammatory dermatoses. Photodermatol Photoimmunol Photomed. 2003;19(4):164–168.
43. Coven TR, Burack LH, Gilleaudeau R, et al. Narrowband UV-B produces superior clinical and histopathological resolution of moderate-to-severe psoriasis in patients compared with broadband UV-B. Arch Dermatol. 1997;133:1514–1522.
44. Storbeck K, Holzle E, Schurer N, et al. Narrowband UVB versus conventional broad-band UV-B in phototherapy for psoriasis. J Am Acad Dermatol. 1993;28:227–231.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





