IJCRR - 7(10), May, 2015
Pages: 51-54
Print Article
Download XML Download PDF
HYSTERECTOMY: A CLINICOPATHOLOGICAL CORRRELATION
Author: V. Arunadevi
Category: General Sciences
Abstract:Objectives: To correlate indications of hysterectomy with the histopathological findings, in order to determine the percentage of preoperative diagnosis that was confirmed on histopathology and to determine the frequency of unexpected pathologies. Methods: A retrospective study of 200 patients who had elective hysterectomy performed for various indications during the study period from January 2014 to December 2014 was conducted. Settings: Karpaga Vinayaga Institute of Medical Sciences and Research Institute. Results: 97.5% of hysterectomies were done for benign indications. The most common pathology identified was Leiomyoma in 32% of cases. Hysterectomies done for UV prolapse showed atrophic endometrium in 62.7% of cases. Other less frequent pathologies identified included endometrial hyperplasia, disordered proliferative phase and endometrial polyps. Conclusion: Histopathological analysis correlated well with preoperative clinical diagnosis for hysterectomy. Benign pathologies were more common than their malignant counterparts. The commonest indication and histological finding in our setting was leiomyoma. The clinical and pathological correlation is 91.8% in case of leiomyoma. Histological diagnosis is considered the definitive method of evaluating tumours.
Keywords: Leiomyoma, Adenomyosis, Hysterectomy
Full Text:
INTRODUCTION
Hysterectomy is the most commonly performed gynecological surgical procedure. It is estimated that over 500,000 hysterectomies are performed each year. The vast majority of these procedures are still performed via an abdominal approach (64%) with vaginal (22%) and laparoscopic (14%) approaches being less common (Jacoby etal1 ., 2009). The Society of Pelvic Reconstructive Surgeons issued guidance on choosing hysterectomy route in 1999. Since then vaginal hysterectomy has again gained favor2,3. The advantages of laparoscopic hysterectomy are shortterm hospital stay and recovery time. A systematic review and meta-analysis reports the average length of hospital stay to be 2 days less (95% CI 1.9-2.2) when compared to abdominal hysterectomy4 . However, a systematic review based on 5RCTs and 4 large case series reported laparoscopic hysterectomy to be more expensive and time-consuming than abdominal or vaginal hysterectomy5 . Laparoscopic techniques are not without risks and are associated with more complications than open operations, notable amongst which are bladder and ureteric injuries5 . Whether to remove the cervix remains unclear in both open and laparoscopic hysterectomy procedures5 . The disadvantages of a subtotal hysterectomy are possible in on-going menstrual bleeding and requirement of continued cervical surveillance (eg. smears)5 . Fibroids are the most common indication (39%) cited for performance of hysterectomy (Whiteman et al6 ., 2008). The purpose of this study is to correlate various indications of hysterectomy with the histopathological examination.
METHODS
The retrospective study analysis of 200 hysterectomy cases over a period of one year from January 2014 to December 2014 was reviewed in Department of OBG. Patient’s age, type of hysterectomy ,indication of surgery as well as true pathological diagnosis were reviewed , analyzed and correlated.
This study was approved by ethical committee.
RESULTS AND ANALYSIS
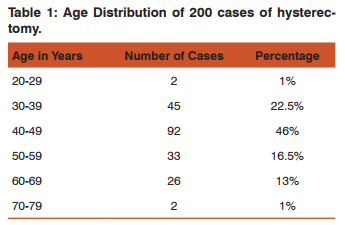
200 hysterectomies were studied. Hysterectomies were distributed over a wide age ranging from 20 years to 80 years. Of this 46% of cases were encountered in 40-49 years, which is the most common age group 22.5% of women were in age group of 30-39 years and 16.5% were 50-59 years. The relationship between age and number of hysterectomies is illustrated in Table 1.
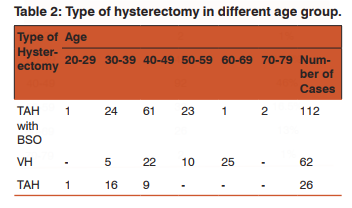
The most common type of hysterectomies was Total Abdominal Hysterectomy with Bilateral Salphingo Ophorectomy (TAH with BSO) and Vaginal Hysterectomy (VH) , followed by Total Abdominal Hysterectomy (TAH). The most common age group for TAH with BSO was 40-49 years and Vaginal hysterectomy was 60-69 years, as shown in Table 2.
The various indications for hysterectomy are depicted in Table 3. 97.5% were benign and2.5% were for malignant indications. Leiomyoma was the most common preoperative clinical diagnosis found in 61 (30.5%) cases, followed by UV prolapse diagnosed in 59 (29.5%) cases. Other benign clinical indications included DUB (20.5%), Adenomyosis (4%), CIN (5.5%), Benign ovarian tumours (5%). 5 hysterectomies were performed for malignant indications which included CA endometrium, CA cervix and CA ovary

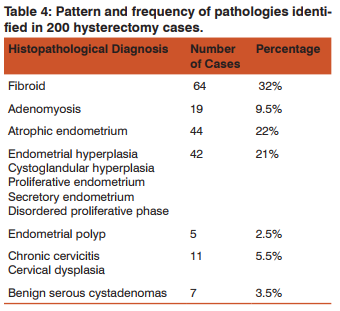
Leiomyoma was the commonest pathology found in 32% of cases as illustrated inTable 4. Hysterectomies for UV prolapse showed atrophic endometrium in 62.7% of cases. Other less frequent pathologies identified included endometrial hyperplasia, disordered proliferative phase and endometrial polyps. 7 cases of Benign serous cystadenomas, 2 cases of ovarian endometriosis and 1 case of hydrosalphix was found. 2 cases of endometrial adenocarcinoma, 2 cases of squamous cell carcinoma of cervix and 1 case of malignant mixed germ cell tumour of ovary was identified.
The final pathologic diagnosis confirmed the clinical indication in 91.8% in cases of leiomyomas, 75% in case of adenomyosis. The 41 cases diagnosed clinically as DUB were pathologically proven as follows: 9 adenomyosis, 8 as fibroid, 8 had endometrial hyperplasia and 2 showed endometrial polyps.
DISCUSSION
Hysterectomy still remains the widely used treatment modality even in developed countries. The complications of hysterectomy are often underestimated. Minor pyrexial morbidity was found in 47% of women after abdominal hysterectomy in the Pinion study with 5% requiring a blood transfusion7 .Common complications after hysterectomy include hemorrahage (2.4%), genitourinary disorders (eg. urinary retention, renal or ureteral injury) (1.9%), urinary tract infection (1.6%) and infection other than that in the urinary tract (1.6%)8 In a retrospective study including over 62,000 hysterectomies, the total incidence of ureteral injury after all hysterectomies was 1.0 of 1000 procedures and only 0.4 of 1000 procedures after total abdominal procedures (Harkki – Siren etal9 ., 1998). It has been shown that hysterectomy increase risk for subsequent stress urinary Incontinence (SUI). The true incidence of SUI caused by hysterectomy remains controversial (Roovers et at.,10 2000) Adhesion after an abdominal operation is very common, infact, 94% of patients develop intra-abdominal adhesions following a laparotomy 11,12. Al-Sunaidi and Tulandi13, studying small bowel obstruction (SBO) after hysterectomy for benign conditions, reported that TAHrelated adhesions accounted for 98% of SBO. The pooled rate for surgical site Infections (SSIs) after abdominal hysterectomy is reported at 1.7% by the National Health care Safety Network but ranged from 1% to 11% (olsen et at., 14 2009). The incidence of vault prolapse after vaginal hysterectomy for prolapse is approximately 12% but only 2% when the indication was other than prolapse15. Larger uteri are associated with a higher complication rate, primarily due to blood loss. When comparing uterine weights of less than 500 g, 500-999g, and greater than 1000g, risk of experiencing blood loss over 500ml, blood transfusion, major organ injury, and hospital readmission all increased as weight of the uterus increased (Unger et al., 16 2002). In 4% of women who die of cancer of the ovary, cervix and uterus hysterectomy should be seen as a life saving as well as life enhancing procedure.17 Hysterectomy has a high patient satisfaction rate because it is curative, usually performed when medical or minimal access management has failed, and repeated procedures or prolonged follow up is not needed. 18, 19-21
CONCLUSION
While confirming the preoperative diagnosis by histopathological examination, high confirmation rates were found for leiomyomas, malignancy and adenomyosis. Out of 41 cases , clinically diagnosed as DUB, histopathological examination revealed leiomyoma in 8 cases, adenomyosis in 9 cases, endometrial polyp in 2 cases.
ABBREVIATIONS
RCT – Randomised Controlled Trial
TAH with BSO- Total Abdominal Hysterectomy with Bilateral Salphingo Ophorectomy
VH - Vaginal Hysterectomy
CIN - Cervical Intraepithelial Neoplasia
DUB – Dysfunctional Uterine Bleeding
SUI - Stress Urinary Incontinence
SBO - Small Bowel Obstruction
SSI - Surgical Site Infection
ACKNOWLEDGEMENT
Author acknowledges the enormous help received from the scholars whose articles have been cited and incorporated in references. Author is also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this articles has been reviewed and discussed.
References:
1. Jocoby VL, Autry A, Jacobson G, et al Nation wide use of laparoscopic hysterectomy compared with abdominal and vaginal approaches. Obstet Gynecol 2009: 114: 1041- 1048.
2. Babalola EO, Bharucha AE, Schleck CD, et al. Decreasing utilization of hysterectomy, a population based study in Olmsted country, Minnesota, 1965-2002. Am J obstetric Gynecol 2007; 196; 214, e1-7
.3. National Guideline Clearing house (NGC). Guideline synthesis; guidelines for determining the route of hysterectomy for benign conditions.
4. Laparoscopic techniques for hysterectomy. National Institute for Health and Clinical Excellence, November 2007.
5. Luesley DM. Obstetrics and Gynaecology. An Evidence – Based Text for MRCOG 2nd ed. Hodder Arnold, 09/2010; 571-2.
6. Whiteman MK ,Hillis SD, Jamieson D, et al. Inpatient hysterectomy surveillance in the united states, 2000-2004. Am J Obstet Gynecol 2008; 31-37.
7. Pinion SB, Parkin DE, Abramovich DR et al. Randomised trial of hysterectomy, endometrial laser ablation and transcervical resection for dysfunctional uterine bleeding .BMJ 1994; 309; 979-983.
8. Spilsbury K, Hammond I, Bulsara M, Semmens JB. Morbidity outcomes of 78, 577 hysterectomies for benign reasons over 23 years. BJOG 2008; 115; 1473-83.
9. Harkki – siren P, sjoberg J, Tiitinen A. Urinary tract injuries after hysterectomy. Obstet Gynecol 1998; 92, 113-118.
10. Roovers JP, van der Vaart CH, van der Bom JG, Heintz AP.Urinary incontinence after hysterectomy. Lancet 2000;356:2012-2013.
11. Tulandi T, Al-Shahrani A, Adhesion prevention in gynecologic surgery . Curr Opin Obstet Gynecol 2005;17:395-398.
12. Ellis H, Moran BJ, Thompson JN et al. Adhesion-related hospital readmissions after abdominal and pelvic surgery; a retrospective cohort study. Lancet 1999;353;1476-1480.
13. Al-Sunaidi M, Tulandi T. Adhesion-related bowel obstruction after hysterectomy for benign conditions. Obstet Gynecol 2006;108:1162-1166.
14. Olsen MA, Higham-Kessler J, Yokoe DS, et al.Developing a risk stratification model for surgical site infection after abdominal hysterectomy. Infect Control Hosp Epidemiol 2009;30;1077-1083.
15. Marchionni M, Bracco GL, Checcuci V et al. The true incidence of vaginal vault prolapse: thirteen years experience, J Reprod Med 1999;44;679-684.
16. Unger JB, Paul R, Caldito G. Hysterectomy for the massive leiomyomatous uterus. Obstet Gynecol 2002;100:1271- 1275.
17. Studd J Hysterectomy A life saving as well as life enhancing operation. Menopause Int 2009; 15:2-3.
18. Lethaby A, Hickey M, Garry R, Penninx J. Endometrial resection / ablation techniques for having menstrual bleeding. Cochrane Database syst Rev 2009;CD001501.
19. A randomized trial of endometrial ablation versus hysterectomy for the treatment of dysfunctional uterine bleeding: outcome at four years. Aberdeen Endometrial Ablation Trials Group. Br J Obstet Gynaecol 1999;106:360-6.
20. Reich H, Ribeiro SC, Vidalia A. Hysterectomy as treatment for dysfunctional uterine bleeding. Baillieres Best Pract Res clin obstet Gynaecol 1999;13:257-67.
21. Ballard L, Lyon DS, Jones JL. Inpatients with menometrorrhagia : etiologies, treatments and outcomes. South Med J 2000;93:571-4.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





