IJCRR - 7(13), July, 2015
Pages: 74-78
Print Article
Download XML Download PDF
LEVEL OF SERUM CREATINE PHOSPHOKINASE IN ORAL SUBMUCOUS FIBROSIS - A BIOCHEMICAL STUDY
Author: Biju Baby Joseph, Shiny George
Category: Healthcare
Abstract:Context: Oral squamous cell carcinomas develop from a premalignant lesion or condition, which are due to a variety of aetiological factors. Early detection of these are necessary to prevent them from developing into carcinomas which can increase the mortality and morbidity. There are a variety of possible aids like histopathology, Hstiochemistry and Enzyme assays in diagnosing these lesions. Histopathology has many limitations which can be overlookd by an enzyme assay technique. Keeping this in mind a study was planned to evaluate the association between serum creatine phosphokinase and a premalignant condition. Aim and objective: To evaluate creatine phosphokinase level in patients with Oral Submucous Fibrosis and to compare it with the normal subjects Methodology: Routine out patients visiting the department of oral medicine and radiology, coorg institute of dental sciences, Virajpet in the age range of 40-60 years old males. They were grouped and samples were collected and sent for analysis. Result: We could not find any statistical significance in the study . Conclusion: A multicentered study consisitng of a large sample is needed to emphasise the importance of creatine phosphokinase as a diagnostic biomarker in Oral Submucous Fibrosis
Keywords: Premalignant lesions, Enzymes, Oral submucous fibrosis
Full Text:
INTRODUCTION
Oral malignancy is widely recognized as the most common cancer in orofacial region.1 It ranks 5th in the world, and in South Asia it ranks 1st in males and 3rd in females among all other cancer. 2 The survival rate oral malignancies are less than 50 %, though treated, hence it is very important to recognise these malignancies at the earliest stage.3 The aetiology of these can be multifactorial and but are strongly related to life style and habits like tobacco chewing, and alcohol, however virus are also proved to be one of the aetiological factor 4 . The oral premalignant lesions and conditions more precisely Potentially Malignant Disorders(PMD) as given by World health Organization (WHO) have got the potential to change into malignancies, when undiagnosed earlier. Few of them are Oral Leukoplakia(OL) and Oral Submucous Fibrosis (OSMF), Oral Lichen Planus(OLP) Erythroplakia and Erythro-leukoplakia. Among these the most common ones are Oral Lichen planus and oral submucous fibrosis, both associated with habits.5 These lesions are clinically and histologically distinct, and have malignant potential. However not all of them transform in to malignant ones.The concept of premalignancy is more suitable to Indian subcontinent owing to the use of tobacco. The damage caused to the oral mucous membrane starts at very early age and added to this any deleterious habit act as adjuvant and pave way for premalignancy. The Potentially malignant disorders if diagnosed early can be treated well to prevent from being grown in to a full blown malignancy and better prognosis of treatment can be achieved when compared to treating a malignant ones.6 Detection of these potentially malignant disorders at the earlier stage and their intervention is very important in preventing them from being transformed in to higher stage. Identification of these depending upon the sites or habit are also important. An early detection all these help to improve the mortality and quality of life of the patient.7 Once the malignant changes have occurred then with our limited resource an impact can be achieved if the right priorities and strategies are established and implemented in treatment strategy. For this to happen an early detection is must.8 There are various diagnostic aids in detecting the premalignant lesions like vital staining , histopathology, VEL scope, Vizilite, saliva , biomarkers7 . Biomarkers help in detecting the earlier stages of malignant transformation and they reveal the early, intermediate and final cellular stage in these lesions9 . Markers like lactic dehydrogenase, phosphohexose isomerise has been found elevated in some cancers. The enzyme creatine phosphokinase is a hypothetize marker for cancer in lung and colon.7 Enzymes are preferred in diagnosis because of their substrate specificity and their activity can be quantified in the presence of other proteins. In each disesase state there is a consequent amount of tissue damage in the involved organ. By finding out the serum level of the enzyme it can act as a diagnostic biomarker.10 The diagnostic value creatine phosphokinase is well documented.It is seen in skeltal muscle, cardiac muscle.Increased levels are noted in myocardial infarction, in muscular dystrophy, in muscle trauma, and in intramuscular injections.Hence an elevation of total creatine phosphokinase in blood suggests muscle or skeltal disease.11 This is also substantiated in another study done by Paola b et al where they did study due to direct and indirect damage of muscle due to various factors. They concluded in a positive significance of creatine phosphokinase in direct muscle damage when compared to indirect damage12.
MATERIALS AND METHOD
Routine out patients visiting the department of oral medicine and radiology, coorg institute of dental sciences, Virajpet in the age range of 40-60 years old males.
METHOD OF COLLECTION
Age, gender, dental status of patient noted down. 20 Patients 20 control were taken after obtaining written consent , detailed case history was taken, and through clinical examination was done and lesions were identified , by experienced oral medicine specialist.
The patients were grouped in to two groups :Group1- having grade 1 –osmf.
Group 2- having grade 2- osmf.
All patient having areca nut chewing habits..
The Inclusion criteria were male patient of age 40-60, and patient willing for the study and treatment thereafter. Whereas the Exclusion criteria were ; Physically and mentally disabled and Patient with history systemic illness.
RESULT
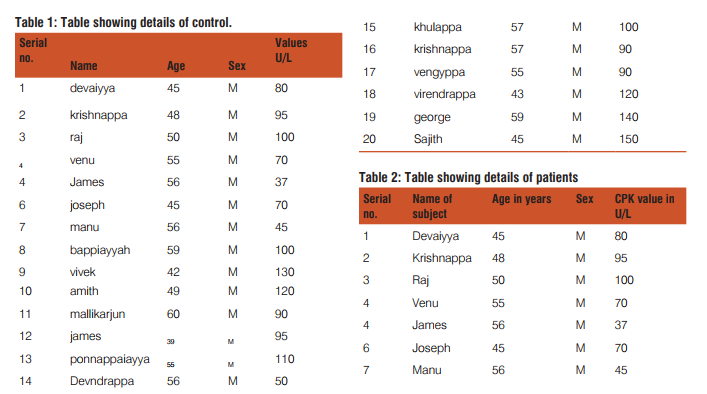
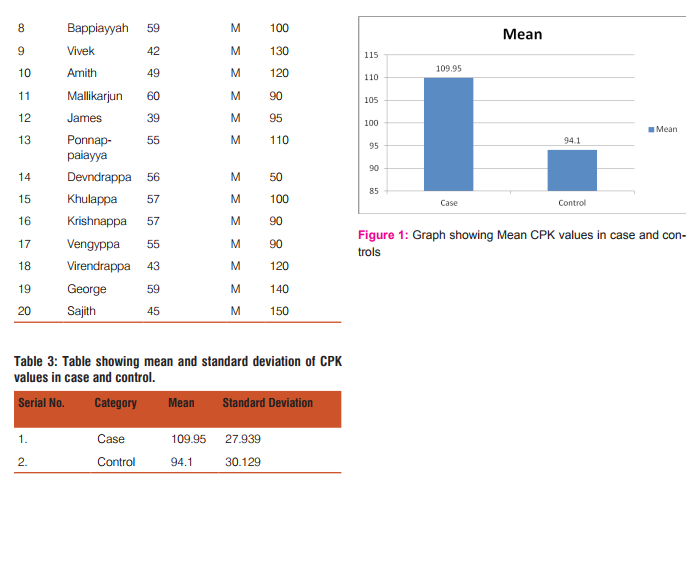
The study had 20 controls and 20 patients in the age group of 40-60 ( table 1 and 2 ). The study was conducted in the Department of Oral Medicine and Radiology in out patient section of Coorg Institute of Dental Sciences. The study showed no statistical significance. The P value was greater (0.598 ). However the mean value showed a slight difference (Table 3 ) between case and control but are with in the normal range.
DISCUSSION
Oral cancer developing from a precancerous lesion is common.According to the literature the deleterious oral habits leads to potentially malignant disorders.The habits such as use of tobacco both in smoking and non-smoking, pan masala, Gutkha, and products which contain areccanut is the main causative agent for potentially malignant disorders. In an Indian preview use of areccanut is the most common agent. This contain certain chemicals which damage the mucosa .The most common damage clinically manifests in the form oral submucous fibrosis.2 Early detection of potentially maliganant disorders can prevent malignant transformation to certain extent. There are several studies done regarding the early detection methods of potentially maliganant disorders namely vital staining, histopathology, and detecting biomarkers. The aim of this study was to evaluate the significance of creatine phosphokinase in oral submucous patients and to compare it with healthy subjects. Oral submucous fibrosis is a precancerous condition characterized by juxtaepithelial inflammatory reaction and progressive fibrosis of the submucosal tissues ie lamina propria and deeper connective tissues(muscle layer). Since it involves the deeper layer as the condition progress the clinical sign is restricted mouth opening. The malignant transformation of oral submucous fibrosis is well documented13 Hence the early detection of this condition is of at most important. Even though it can be clinically diagnosed, the severity of dyspalsia cannot be judged. Hence an alternate method to detect the severity and dysplastic changes is necessary, which are reasonable for systemic involvement. A new enzymatic approach for diagnostic and prognosis of the disease is documented in a study has been done bySpoorthy et al 7 .The diagnostic and prognostics value of creatine phosphokinase as biomarker in other systemic disease are well documented. creatine phosphokinase is an enzyme which is released due to muscle damage in different systemic diseases. Hence this is used as biomarker to find out the extent of muscle damage or the progress of a disease. The importance of biomarkers in muscle damage is documented in a study done by Brancaccio et al. The author recommends to use these biomarkers for muscle stress, and damage12. In a study done by Ravi et al found appositive correlation between creatinie phosphokinase and potentially malignant disorders 7 . In a study done by Partovi et al to find out the impaired microcirculation in systemic sclerosis, found out that the these patients had abnormal elevation of creatine phosphokinase, and other factors14. The studies done by AZl Gani et al, in patients with acute myocardial infarction, found positive coorelation with these patients 15,16 But Joseph et al did their study on colon cancer patients to find out the significance of cretine phosphokinase and got a positive correlation 17. Arthur et al did their study on marathon runners to find the correlation between creatine phosphokinase and exercise. Their study was based on time gap and got a positive correlation between creatine phosphokinase and running18. Zarghami et al found the prognostic value is much less in ovarian cancers due to the drugs administered did not show any metabolism related values19. The exact mechanism for enzyme release is not clear, but some sort of muscle tissue damage can change the serum value of creatine phosphokinase which can be substantiated by the above studies. Since there is the release these enzymes the muscle damage can be assessed at very earlier in different diseases. Out of the various conditions studies done in patients with myocardial infarction showed more significance nevertheless colon cancers ,renal problems also showed significance. The significance of potentially malignant disorders like oral leukoplakia, oral submucous fibrosis showed statiscal significance e in a study done by Spoorthy et al.17,7 But the alteration of creatine phosphokinase level in a marathon runners as the study done by Arthur says it could be related to rhabdomyolysis which is due to over use of the muscle. In a patient developing oral submucous fibrosis due to excessive chewing over many years can be explained against the fact of over use of the buccal musculature. This is also substantiated by the study done by Dessem et al where he studied the muscle response to injury or over use over a long period of time, the levels of creatine phosphokinase are altered in different muscles in different parts of the body 20. The primary factor for muscle damage is due to proteolysis. IL 6, IL1, ANS TNF ALPHA are found increased in submucous fibrosis patients, which are factors which help in proteolysis.21,7 These cytokines are elevated due to activated T –lymphocytes present in the premalignant tissues7 . Keeping this view in mind we designed a study to find out the significance of creatine phosphokinase in oral submucous fibrosis patients. Our study had total 20 patients in the age group of between 40-60 male patient without any other systemic disease, who had habits of chewing of areca nuts. They had no clinical signs of anemia. We did not get a statistical significance between creatine phosphokinase to oral submucous fibrosis against as documented in other literature 7 (Table 1,2,and 3) However we could not trace a literature stating such an increase of creatine phosphokinase in oral submucous fibrosis. This could be due to the difference in pathophysiology of oral submucous fibrosis and other diseases like myocardial infarction and colon cancer, where in the creatine phosphokinase showed a significant correlation 16 But our study shows a mild difference in levels of creatine phosphokinase between normal subjects and oral submucous fibrosis patients.( Figure 1 ) The high range of P value(P value 0.598 ) could be substantiated by the reason that either too low sample, single centered study, and the subject’s severity of the condition of oral submucous fibrosis ie the dysplastic changes could be mild resulting in a no or subclinical muscle damage. In oral submucous fibrosis there is juxtaepithelial inflammatory reaction continued by activation of collagen production pathway leading to deposition of type 1 collagen fibres where as in myocardial infarction there is overuse of the cardiac muscle in a very short time period, which finally results in damage of the heart muscle. This damage causes the alteration in MB part of creatine phosphokinase enzyme. This is substantiated in the study conducted by Paola b et al on muscle damage from direct and indirect aetiological factors.12 Whereas in fibrosis there is reduction in blood supply in the region resulting in reduced nutrient flow, reduced immunity, to the region just as in systemic sclerosis as demonstrated by Partovi et al study14,22 Over a period of time there can be complete fibrosis and loss of activity of the muscle leading to improper diet, nutrition, minerals and thereby poor quality of life.
CONCLUSION
From this study we conclude that there is no definite underlying biochemical alteration with respect to enzyme creatine phosphokinase as a diagnostic marker for oral submucous fibrosis and this biomarker is not reliable.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholers who articles are cited and included in reference of this manuscript. The authors are also greateful to authors of authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Wei Liu†, Yu-Feng Wang. Malignant transformation of oral leukoplakia a retrospective cohort study of 218 Chinese patients. BMC Cancer , 2010; 10:685.
2. Sunil P.R ,et al. Current Trends in Diagnosis of Oral Cancer and Premalignant Lesions: An Update. JDSOR, July-September 2014;5(3):120-124.
3. K. Venkatakrishna, V. B. Kartha. HPLC-LIF for early detection of oral Cancer. CURRENT SCIENCE, February 2003 : 84( 4) 25
. 4. Crispian scully, Updates. November 2010,9 (4).
5. Syed Salman H , S. Nazia Ambreen,. The clinical and Morphological study of 75 cases of oral premalignant lesions. J of Evolution of Med and Dent Sci. February 2105,4 (14) 2278-4748.
6. Goyal D1, Goyal. An update on precancerous lesions of oral cavity. IJMDS. January 2013; 2(1).
7. Spoorthi B R , Vidya M. serum Creatinine Phosphokinase : A Potential diagnostic tool for oral premalignant lesions ?- A histopathological biochemical study. Indian J Stomatol.2011 ;2 (2): 86-90.
8. M. KRISHNAN NAIR, CHERIAN VARGHESE. Cancer: Current scenario, intervention strategies and projection for 2015. NCMH Background Papers·Burden of Disease in India.
9. Sonalee Shah, Manpreet Kaur. Biomarkers and chemopreventives in oral carcinogenesis and its prevention. Journal of Oral and Maxillofacial pathology.Jan- April 2014 18 (1).
10. Thiagarajan Hemalatha, Thaiagamoorhty Uma Mahashawary. Enzymes in clinical Medicine – An Overview. Indian Journal of Experimental Biology. October 2013. 51:777-788.
11. Willie L. Ruff, PhD, Roger Worrell, MD. Diagnostic Value of Creatine Phosphokinase (CPK) lsoenzymes in the Absence of Elevated Total CPK.Journal of the National Medical Association. 1979.71 (4).
12. Paola Brancaccio1, Giuseppe Lippi, Biochemical markers of muscular damage. Clin Chem Lab Med 2010;48(6).
13. Michael C Herbst , cansa, February 2015.
14. Sasan Partovi1, Anja-Carina Schulte, Impaired skelet al muscle microcirculation ic systemic sclerosis, Arthritis Research & Therapy 2012, 14:R209
15. Fethi Abed ALGani. Significance of Total Creatine Kinase and Creatine kinase-MB Levels In Patients With Acute Myocardial Infarction. Int J Biol Med Res. 2011; 2(3): 762-765.
16. A. F. Smith, D. Radford. Creatine kinase MB isoenzyme studies in diagnosis of myocardial infarction. British Heart Journal, 1976, 38, 225-232
17. J Joseph’, A Cardesa2 and J Carreras1. Creatine kinase activity and isoenzymes in lung, colon and liver carcinomas. British Joumal of Cancer (1997) 76(5), 600-605
18. A. ARTHUR J. SIEGEL, M.D., LAWRENCE M. SILVERMAN. Creatine Kinase Elevations in Marathon Runners: Relationship to Training and Competition. TIHEYALE JOURNAL OF BIOLOGY AND MEDICINE 53 (1980), 275-279
19. Nosratollah Zarghami.Prognostic value of BB isoenzyme in epithelial overian carcinoma.the Canadian Journal of Oncology, September 19915 :5 (3).
20. Dean Dessem1, 2 and RichardM, Lovering. RepeatedMuscle Injury as a Presumptive Trigger for ChronicMasticatoryMuscle Pain, Pain Research and Treatment, 2011.
21. V V Kamath,1 K Satelur,1 and Y Komali. Biochemical markers in oral submucous fibrosis: A review and update. Dent Res J (Isfahan). 2013 Sep-Oct; 10(5): 576–584.
22. Rasika Priyadharshani Ekanayaka. Oral Submucous Fibrosis: Review on Mechanisms of Pathogenesis and Malignant Transformation. J Carcinogene Mutagene 2013, S5.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





