IJCRR - 7(19), October, 2015
Pages: 40-42
Date of Publication: 10-Oct-2015
Print Article
Download XML Download PDF
BILATERAL UNDESCENDED TESTES : ITS CLINICAL SIGNIFICANCE
Author: Jeneeta Baa, J. S. Prusti
Category: Healthcare
Abstract:Cryptorchidism is a condition in which one or both the testes have not reached the scrotal sac. During routine dissection of an unclaimed middle aged male cadaver, we found bilateral undescended testes. The testes were located at the superior inguinal ring and both the scrotal sacs were empty. An empty scrotum raises suspicion of a number of testicular anomalies. Early diagnosis and intervention is necessary as testicular variations can result in many diseased conditions like testicular torsion, tumors and cancers
Keywords: Superficial inguinal ring, Retractile testis, Empty scrotum, Infertility
Full Text:
INTRODUCTION
Testes are a pair of male gonads which begins its development at 6 weeks of intrauterine life in the posterior abdominal wall and is completed by the 5th month of intrauterine life. Differential growth of the embryo in intrauterine life causes certain organs to ascend and some to descend for functional reasons. During descent into the scrotal sac the testis can be arrested anywhere along its normal path. Cryptorchidism is a condition in which one or both the testes have not reached the scrotal sac. If it deviates from its normal path of descent, the condition is known as ectopic testis [1].
CASE REPORT
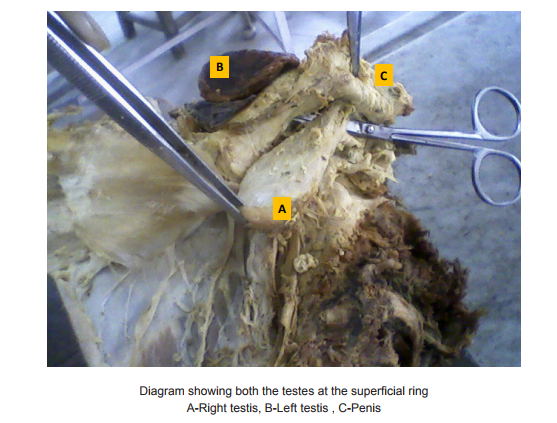
During routine dissection, we noted bilateral undescended testes in an approximate 50 years old male cadaver. Both the testes were found at the superficial inguinal ring. The dimensions observed were : Right testis : length-5.5 cm, width-3 cm, thickness-1.3 cm and Left testis: Length-5.7cm, width-3.5 cm, thickness-2 cm. Both the scrotal sacs were found to be empty.
DISCUSSION
The descent of testes occurs in two phases under the control of different factors [2]. The anti-mullarian hormone influences the trans-abdominal phase whereas the gubernaculum guides the inguino-scrotal phase. The testis appears in the iliac fossa by the fourth month of fetal life, in the deep inguinal ring at the seventh month, in the inguinal canal during eighth month and in the scrotum at birth [1, 3]. According to a study in 223 patients, the most common abnormal location was the high scrotal position in 44% of patients, in 26% it was the superficial inguinal pouch, in 20% at the inguinal canal and in 10% it was in the abdomen [4]. In the present case both the testes were found arrested at the superficial inguinal ring. If undescended at birth, the testis completes its descent in the first three months of life. Therefore 3-5% of the full term babies with undescended testes show a reduced incidence of 0.8% by three months of age [5]. Incidence of undescended testes is approximately 1 in 1000 to 1 in 2500 [6]. Factors like exposure to maternal estrogen in fetal life, deficiency of androgen, inadequate internal secretions, genitofemoral nerve function failure, low intraabdominal pressure and lack of differential growth are also known to cause the condition [7].The commonest cause is believed to be a defect in prenatal androgen secretion secondary to either deficient pituitary gonadotrophin stimulation or low production of gonadotrophins by placenta[8]. Cryptorchidism is a part of several chromosomal anomalies like Prader willi syndrome, Klinefelter syndrome, Laurence moon-biedl syndrome, Lowe syndrome. In trisomy13 and trisomy15, 50% of the male infants have undescended testes whereas it is less frequently seen in trisomy18 and trisomy21 [9]. It is also associated with inguinal hernia, renal anomalies and other male genital organ deformities. An empty scrotum can be due to testicular anomalies like absent testis, undescended testis, ascended testes, nonpalpable testes, ectopic testis, and retractile testis. Non-palpable testes, if bilateral are difficult to diagnose. In such a case intersex anomalies must be ruled out and possibility of anorchia must be considered [9]. Approximately 20% of cryptorchid testes cannot be palpated on physical examination as they are associated with a patient processes vaginalis are thus show reasonable degree of mobility [10]. A retractile testis is due to an overactive cremasteric reflex. It’s diagnosis is made if the testes that is undescended has earlier been seen in the scrotum. Such reflex contraction of the genitofemoral nerve due to tactile stimulation is present in all boys after age 2 years [11].So these patients belong to an age group of 2-6 years. An ascended testes results from limited ability of the spermatid cord to elongate. Iatrogenic ascent is also a common finding in upto 10% cases after repair of indirect inguinal hernia and after liposuction of the prepubic fat pad for buried penis repair [12].
CONCLUSION
Men with undescended testis have a lower sperm count, poor quality of sperms and low fertility rates [1]. In the present case we could not get any family history as it was an unclaimed body. Undescended testis have higher chances of development of germ cell tumor than the normal and the incidence increases with advancement of age [13 ].Early detection of the cause by imaging techniques like ultrasonography, CT scan , MRI ,spermatic venography and laparoscopy therefore becomes necessary . Surgical intervention (Orchiopexy) as early as six month of age can prevent testicular cancer. Hormonal therapy can distinguish a retractable testes from a congenital undescended testes. In addition, it is equally beneficial because hormone stimulation may restore a normal testicular function after surgery. It is often assumed that a descended testes remains descended permanently. However there are documented cases in which previously descended testes have been found to ascend permanently out of the scrotum [14].The mechanism behind this ascent is unknown. Clinicians must therefore be aware that finding a scrotal testes does not rule out the future possibility of its ascending out again.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.

References:
1. Keith L. Moore, T.V.N.Persaud- The Urogenital System. In:chapter 12, The Developing Human-Clinically Oriented Embryology, 8th ed. Philadelphia Saunders Inc,2008: 279-281.
2. Kolon TF, Patel RP Huff DS(2004). “Cyptorchidism:diagnosis, treatment, and long-term prognosis”. Urol. Clin. North Am. 31(3):469-80, viii-ix. doi:10.1016/j.ucl.2004.04.009.PMID 15313056.
3. Susan Standring- Male Reproductive system. In:Chapter 97, Neil R. Borley editor-Gray’s Anatomy. 39th ed. Edinburgh: Elsevier Churchill Livingstone, 2005: 1306.
4. Scrorer CG,Farrington GH:Congenital deformities of the testis and epididymis. NewYork;Appleton-Century-Crofts,1972.
5. Steven G Docimo, Richard I Silver and William Cromie-The Undescended Testicle: Diagnosis and Management. The American Academy of Family Physicians Nov 1 2000 ;2047.
6. Pinczowski D, McLaughlin JK, Lackgren G, Adami HO, Persson I. Occurrence of testicular cancer in patients operated on for cryptorchidism and inguinal hernia. J Urol. 1991:146:1291-4.
7. A.K. Datta-The Urogenital System. In Chapter 16-Essentials of Human Embryology. 5th ed.Kolkata:Current Books International Publication ,2005:238-241.
8. Husmann DA, Levy JB. Current concepts in the pathophysiology of testicular undescent. Urology1995; 46(2): 267-276.
9. Micropenis, Hypospadias,and Cryptorchidism in Infancy and childhood. Kenneth L Becker (ed).Principles and Practice of Endocrinology and Metabolism, 3rd ed. USA: Lippincott Williams and Wilkins; 2001. pp. 912.
10. Mital V K, Garg Brijendra K. Undescended testicle. The Indian Journal of Pediatrics 1972; 39(5):171-174.
11. Caesar RE,Kaplan GW.The incidence of the cremasteric reflex in normal boys.J Urol 1994;152:779-780.
12. Kaplan GW.Iatrogenic cryptorchidism resulting from hernia repair. Surg Gynecol Obstet 1976;142:671-672.
13. Moller H, Cortes D, Engholm G, Thorup J (1998).Risk of testicular cancer with cryptorchidism and with testicular bio. PMC: 28664. psy: cohort study. BMJ 317 (7160): 729. PMID 9732342.
14. Mayr J, Rune GM, Holas A, Schimpl G, Schmidt B, Haberlik A. Ascent of the testis in children. European Journal of Pediatrics 1995; 154(11):893 .
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





