IJCRR - 8(1), January, 2016
Pages: 01-05
Print Article
Download XML Download PDF
RETROSPECTIVE ANALYSIS OF CHOLECYSTECTOMY PERFORMED IN AN INSTITUTION FOR LOWER SOCIOECONOMIC POPULATION IN INDIA
Author: Tanweer Karim, Subhajeet Dey, Rabishankar Singh, Vivek K. Katiyar
Category: Healthcare
Abstract:Background: Gallstones are common in Indian population.Laparoscopy requires longer and steeper learning curve and proper patient selection. Patients belonging to lower socioeconomic group usually present late, develop one or the other complications of cholelithisis prior to surgery and expected to have higher conversion rate, per-operative and post-operative complications. Aims: To study safety and efficacy of laparoscopic cholecystectomy in patients of cholelithiasis by comparing with results of open cholecystectomy in terms of use of post-operative analgesia, operative Time, post-operative hospital stay, morbidity and mortality. Material and Method: Patients operated for gallbladder stone betweenJanuary 2013 and August 2015were retrospectively analyzed in terms of demographic profile, clinical presentation, procedureperformed and its findings, operating time, conversion rate, postoperative pain and analgesic requirement, postoperative hospital stay and complication. Results: Cholecystectomy was performed in 630 patients between January 2013 and August 2015. 368 patients were operated laparoscopically and 232 patients by open method. It comprises of almost 25 percent of major operations performed during this period, 75.8% were females and 9 of them were less than 15 years of age. The mean operating time during 2013 for laparoscopic and open Cholecystectomy was 68.37 minutes and 66.20 minutes, decreased to 46.27 minute and 53.33 minute during 2014-15, respectively. Intraoperative cholangiography was not required in any case. Conclusion: Cholelithiasis is relatively common in India even in lower socio-economic group. Dietary habits and obesity do not appear as contributing factor.Laparoscopy has better visibility, access and operating time than open cholecystectomy. Complications rate is negligible even in difficult gallbladders, if proper planning is done with ultrasonography and liver function test 24 hours prior to surgery.
Keywords: Laparoscopic cholecystectomy, Open cholecystectomy, Cholelithiasis, Obstructive jaundice, Pancreatitis
Full Text:
INTRODUCTION
Laparoscopic cholecystectomy is a revolutionary change in the treatment of patients with gallbladder stones. Mouret introduced laparoscopic cholecystectomy in 1987[1]. It has rapidly replaced open cholecystectomy as the standard treatment. Advantages of laparoscopic cholecystectomy include reduced hospitalization, decreased morbidity, short recovery time, and better cosmesis[2].Laparoscopic cholecystectomy though safe and effective, yet can be difficult at times. Various problems faced are difficulty in creating pneumoperitoneum, accessing peritoneal cavity, releasing adhesions, identifying anatomy, anatomical variation and extracting the gall bladder. Laparoscopic cholecystectomy with these problems along with time taken more than normal is considered as difficult.Pre-operative prediction of a difficult laparoscopic cholecystectomy can help the patient as well as the surgeon prepare better for the intra-operative risk and the risk of conversion to open cholecystectomy.
AIMS To study safety and efficacy of laparoscopic cholecystectomy in patients of cholelithiasis by comparing with results of open cholecystectomy in terms of use of post-operative analgesia, operative time, post-operative hospital stay, morbidity, mortality and factors responsible for conversion.
MATERIAL AND METHOD 630 Patients underwent cholecystectomy between January 2013 and August 2015.Since laparoscopic cholecystectomy has been considered as gold standard we offered this option to thepatients except in cases of gallbladder mass, post ERCP and CBD stenting, cardio-respiratory diseases (ASA grade III/ IV) or where patient’s choice was for open cholecystectomy. Patients have been managed by single unit of department of Surgery, ESIC PGIMSR, Basaidarapur, New Delhi, India, an organization which provides social security and healthcare services to lower socio-economic population.Record sheets of 630 patients operated between January 2013 and August2015 were retrospectively collected. Information regarding demographic profile, clinical features, laboratory and radiological investigations, operating procedure and findings, operating time, Conversion rate, postoperative pain and analgesic requirement, postoperative hospital stay and complication were filled in the proforma. Results were statistically analysed and compared with similar studies.
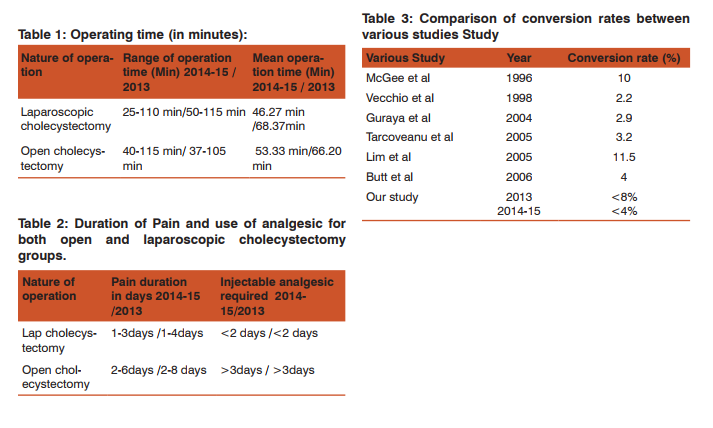
RESULTS 630 patients of cholelithiasis were operated during January 2013 and August 2015. Out of 630 patients,368 were operated laparoscopically and procedure was completed without conversion. 232 patients had undergone open cholecystectomy and 30 patients had been converted to open cholecystectomy after starting laparoscopically(Figure1). These patients were aged between 8years to 87 years with mean of 42 years, 477(75.8%) females and 153(24.2%) males. Nine of them were less than 15 years of age. The mean operation time during 2014-15 for laparoscopic cholecystectomy is 46.27 minute and 53.33 minute for open cholecystectomy. The mean operating time during 2013 for laparoscopic and open cholecystectomy was 68.37 minutes and 66.20 minutes, respectively (Table 1). The number of laparoscopic cholecystectomy performed during 2014-15 was 240 and mean operating time was46.27 minutes [Median-43+43/2=43, Range=85 and Mode=45]. During the same period total number of open cholecystectomy was 160 and mean operating time was53.33 minutes [Median was 45+45/2=45, Range=79 and Mode=45]. The number laparoscopic cholecystectomy during 2013 was 133, Mean operating time was 68.37 minutes [Median=66, Mode=65,66 and Range=65].
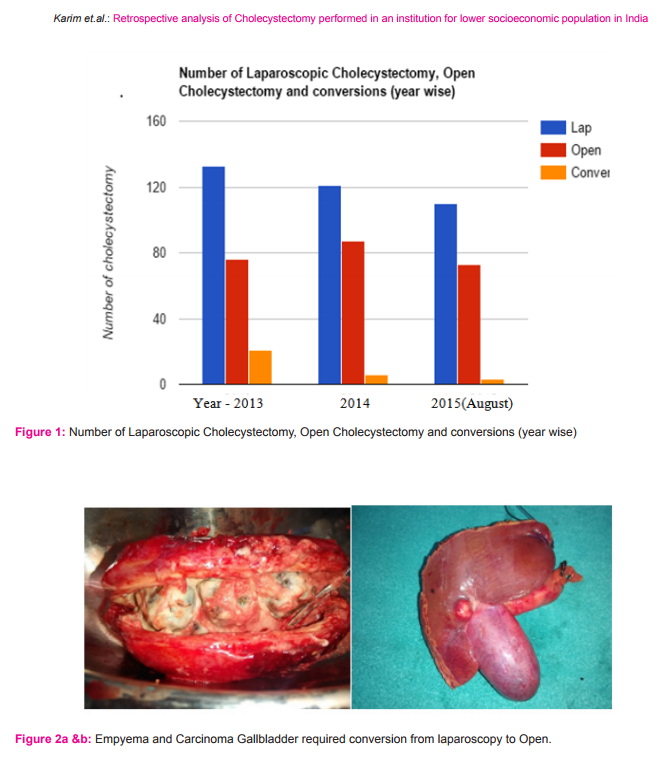
During same period the number of open cholecystectomy was 76 and mean operating time was 66.20 minute [Median=65+66/2=65.5, Range=68.42 and Mode=66]. Total number of laparoscopic cholecystectomy converted to open were 21, 6 and 3 during 2013, 2014 and 2015, respectively. Laparoscopic cholecystectomy was converted to open cholecystectomy in 13 grossly thickened gallbladders not amenable to grasp, 6 cases of contracted gallbladder post ERCP, 5 cases with previous upper abdominal surgery and adhesions all around, 3 cases of suspected carcinoma gallbladder and 3 cases of Mirrizi Syndrome(Figure 2a, 2b). It has been observed that duration of post-operative pain and analgesia required were significantly lesser in laparoscopic cholecystectomy group than open cholecystectomy group. The use of Injectable analgesics in cases of laparoscopic cholecystectomy was maximum for 2 days and it was never less than 3 days in cases of open cholecystectomy(Table2).
Bile leak was present in 3 cases of laparoscopic cholecystectomy during 2013 and one case in 2014. Two of them had leak from cystic duct stump due to distal common bile duct stone. One patient had minor leak from injury to right hepatic duct and one had tear at the confluence of cystic duct and common hepatic duct. MRCP (Magnetic resonance cholangiopancreatography) followed by ERCP (Endoscopic retrograde cholangiopancreatography) and stenting was done in all the cases and flat drain was already placed during surgery. They all recovered within a week time and their stent were removed later. Three patients of open cholecystectomy had minor biliary leak without demonstrable extrahepatic biliary injury on MRCP.
Two patients were diagnosed as cases of Dubin Jonson Syndrome, suspected because of abnormal dark color of liver, hyperbilirubinemia, normal liver enzymes and histopathology has not corroborated with other liver pathology. Wound infection was present in 13 cases of open cholecystectomy only. Therefore, rate of complication and conversion has apparently decreased with better planning and experience. Post-operative hospital stay for laparoscopic group was 2.56 days(Range 1-6 days), whereas it was 3.86 days with range of 2-10 days in open group. Common comorbid conditions were diabetes mellitus, hypertension and hypothyroidism. Majority of cholelithiasis patients have grade 1 or II fatty liver on ultrasonography. However, their dietary habits do not show any specific pattern.
DISCUSSION Very few operations have changed the thinking and operating habits of surgeons as quickly as laparoscopic cholecystectomy. This technique of small incision for cholecystectomy has shown good result in terms of reducing pain and morbidity and paved the way for use of minimal access surgery. Laparoscopic cholecystectomy was first performed in Lyon, France in March 1987 by Philippe Mouret, a general surgeon.[1-4]. The extent to which the surgical incision contributes to morbidity and mortality is well established. Sufficient time has elapsed since the first laparoscopic cholecystectomy was performed.
Most surgeons have passed through the learning curve phase of their experience and have now settled into established patterns of activity. There are studies which show thatthe natural history of incidentally discovered gallstone is not only benign but even when they do develop complications; it is usually preceded by at least one episode of biliary pain and longer the stones remain asymptomatic, the less likely it is that complications will occur. In about 30%, patients who have had pain do not have further episodes of pain. Thus, for persons with asymptomatic gallstones, the natural history is so benign that not only treatment but also a regular follow-up is not recomrnended[5-6].
However, our experience with longstanding cases of cholelithiasis isdifferent and more often than not they present with one or the other complication preoperatively and pose difficulty during surgery. Laparoscopic cholecystectomy changed the view of the surgeons and the patients towards asymptomatic gallstones. After the introduction and widespread use of laparoscopic cholecystectomy, a significant change has been observed possibly due to the attitude of surgeons to relax the indication of surgery, including for asymptomatic gallstone, resulting in an increase in cholecystectomies worldwide. Laparoscopic cholecystectomy in young patients with uncomplicated, asymptomatic gallstones is safe with greater patient acceptance, and this approach in early age eliminates the need for problematic surgery at a later date when the patient is older, with associated diseases or with complications [7-10].
The chance of slipping into CBD is high and complications like obstructive jaundice, cholangitis and pancreatitis are likely [11]. Conversion rates in laparoscopic cholecystectomy ranges from 3% to 15% in well trained hands. In our series composite conversion rate is less than 8%during 2013 which has gone down further to less than 4 percent during 2014-15(Table 3). The frequency of bile duct injury is 0.1 % to 0.2% for open cholecystectomy and 0.3% to 0.6% for laparoscopic cholecystectomy. Two most common reasons for conversion are dense upper abdominal adhesions and thickened gall bladder wall that precludes grasping and elevation with grasper.
Common risk factors for conversion are male gender, obesity, cholecystitis (especially after 48 to 72 hours after onset of symptoms) and choledocholithiasis. Most conversions happen after a simple inspection or a minimum dissection, and the decision to convert should be considered as a sign of surgical maturity rather than a failure. Conversion should be opted for in the beginning and at the time of recognition of a difficult dissection rather than after the occurrence of complication. It is vital for the surgeons and patients to appreciate that the decision to go for conversion is not failure but rather implies safe approach and sound surgical judgment. It is therefore mandatory to explain the patients about possibility of conversion to open technique at the time of taking consent for laparoscopic cholecystectomy [12-13].
Postoperative pain is less compared with open traditional cholecystectomy. However, overall pain after laparoscopic cholecystectomy carries a high inter individual variability in intensity and duration. Pain is most intense on the day of surgery and on the following day and subsequently declines to low levels within 3–4 days. Wound infection in open procedure is 3 times the laparoscopic procedures. Jatzko et al in their study observed that complications rate is lower in laparoscopic cholecystectomy group (0.3%) as compared to open cholecystectomy group (5.1 %). Barkun JS et al in a study also observed that number of complications in laparoscopic cholecystectomy were significantly less than number of complication in open cholecystectomy. Laparoscopic surgery could increase the morbidity and mortality of surgery particularly in elderly patients with limited cardiopulmonary reserve.
Laparoscopic surgery has been theoretically associated with compounding cardiac problems because the intra-abdominal pressure coupled with head up position results in pooling of blood in legs, reduced venous return, hypotension and increased tendency to develop venous thrombosis. Pressure effects of Carbon dioxide gas insufflated, may have effect on venous return, the heart rate and rhythm, basal lung expansion, carbon dioxide retention and acidosis[14-15].
CONCLUSION Difficult laparoscopic cholecystectomy is relatively common in India even in lower socio-economic group. All patients should undergo ultrasonography of abdomen and liver function estimation a day prior to surgery in order to assess gallbladder and common bile duct status and plan accordingly. There is a need to stick to maximum time limit in difficult cases to avoid complications due to surgery or prolonged anesthesia. During the study period operation time for laparoscopic cholecystectomy has shown a tendency to become shorter and conversion rate has shown a decreasing trend probably due to better planning and experience.
ACKNOWLEDGEMENT Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/ editors/ publishers of those articles, journals and books from where the literature for this article has been reviewed and discussed.
Conflict of interest: None
Source of Funding: None
References:
1. Mouret P. From the first laparoscopic cholecystectomy to frontiers of laparoscopic surgery; the future perspective. Dig Surg. 1991;8:124–125
2. Ellis H. John Stough Bobbs: father of gall bladder surgery. British journal of hospital medicine London England 2005. 2009;70(11):650.
3. Traverso LW. Carl Langenbuch and the first cholecystectomy. [Internet]. American journal of surgery. 1976. p. 81–2.
4. Paulino-Netto A. A review of 391 selected open cholecystectomies for comparison with laparoscopic cholecystectomy. American journal of surgery. 1993; 166 (1):71–3.
5. Cheslyn-Curtis S, Russell RC. New trends in gallstone management. The British journal of surgery. 1991;78(2):143–9.
6. Villanova N, Bazzoli F, Taroni F, Frabboni R, Mazzella G, Festi D, et al. Gallstone recurrence after successful oral bile acid treatment. A 12-year follow-up study and evaluation of long-term post dissolution treatment. Gastroenterology. 1989;97(3):726– 31.
7. Escarce JJ, Chen W, Schwartz JS. Falling cholecystectomy thresholds since the introduction of laparoscopic cholecystectomy. JAMA 1996;91(20):2653–4.
8. McSherry CK, Ferstenberg H, Calhoun WF, Lahman E, Virshup M. The natural history of diagnosed gallstone disease in symptomatic and asymptomatic patients. Annals of Surgery. 1985;202(1):59–63.
9. Lam CM, Murray FE, Cuschieri A. Increased cholecystectomy rate after the introduction of laparoscopic cholecystectomy in Scotland. Gut. 1996;38(2):282–4.
10. Jani K, Rajan PS, Sendhilkumar K, Palanivelu C. Twenty years after Erich Muhe: Persisting controversies with the gold standard of laparoscopic cholecystectomy. Journal of Minimal Access Surgery; 2006;2(2):49–58. A
11. Thompson JS, Philben VJ, Hodgson PE. Operative management of incidental cholelithiasis. American journal of surgery. 1984;148(6):821–4.
12. Alponat A, Kum CK, Koh BC, Rajnakova A, Goh PM. Predictive factors for conversion of laparoscopic cholecystectomy. American journal of surgery 2002;21(3):254–8.
13. Domínguez LC, Rivera A, Bermúdez C, Herrera W. Analysis of factors for conversion of laparoscopic to open cholecystectomy: a prospective study of 703 patients with acute cholecystitis. Cirugia Espanola. 2011;89(5):300–6.
14. Barone JE, Lincer RM. Correction: A prospective analysis of 1518 laparoscopic cholecystectomies. The New England Journal of Medicine. 1991. p. 1517–8.
15. Kane RL, Lurie N, Borbas C, Morris N, Flood S, McLaughlin B, et al. The outcomes of elective laparoscopic and open cholecystectomies. Journal of the American College of Surgeons. 1995. p. 222–3.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





