IJCRR - 8(2), January, 2016
Pages: 33-35
Print Article
Download XML Download PDF
RELATIONSHIP BETWEEN CLINICALLY PALPABLE AXILLARY LYMPH NODE AND HISTOLOGICAL POSITIVITY FOR METASTASIS AND MANAGEMENT IN BREAST CANCER PATIENTS
Author: Deepak David S., Sadhan Kumar CH, T. Tirou Aroul, Robinson Smile
Category: Healthcare
Abstract:Aim: The aim of the present study was to find out the relationship between clinically palpable axillary lymph node and histological positivity for metastasis in patients with breast cancer. Method: This is a prospective study of 50 patients who underwent mastectomy with axillary clearance between august 2007 to august 2009 were evaluated. The clinically palpable lymph nodes, number of lymph node retrieved and histological positivity were studied. Results: Out of 50 patients, in 31(62%) patients axillary lymph node were palpable. The number of lymph nodes retrieved varied from 3-13. Among these patients with clinically palpable axillary lymph nodes, in 87% of patients these lymph nodes showed metastasis. Conclusion: Routine Axillary Lymph node dissection (ALND) in clinically node positive patients is useful for determining histological status and also as a therapeutic procedure.
Keywords: Axillary lymph nodal status, Routine Axillary Lymph node dissection
Full Text:
INTRODUCTION
Many studies have proved that axillary lymph nodal status is the most important prognostic indicator in breast cancer and influences the treatment pattern. Axillary lymph node dissection offers excellent loco-regional control and improves overall survival1 . It has seen reported that 30 % of the patients with clinically palpable lymph node proved to be negative and 30 % of the patients with clinically negative have node involvement by histology on axillary dissection2 . Ultrasound guided fine needle aspiration or core needle biopsy has reported a positive result only in 40 percent of axillary node metastasis3 . Sentinel lymph node biopsy (SLNB) has become a routine during the last decade and the recent guidelines recommend removal of clinically palpable axillary lymph nodes irrespective of SLNB results 4 . In 50 breast cancer patients clinically palpable ipsilateral axillary lymph nodes were studied for histological positivity after mastectomy with level II axillary clearance.
Patients and Methods Between August 2007 to August 2009, 50 consecutive patients with breast cancer presented to medical college were included in this study. An informed consent was obtained from each patient and approval of the Ethics committee of this institute was obtained before starting this study. Clinical evaluation with detailed history and physical examination including primary tumour size and axillary nodal status were carried out. Modified radical mastectomy or total mastectomy with level II axillary dissection, were carried out and follow up based on this standard protocol. Parameter studies were histology of the primary, number of nodes retrieved and number of nodes showed metastasis. Statistical test included Pearson’s R test for number nodes retrieved and involved. Chi - square test for clinically palpable lymph nodes and histological positivity.
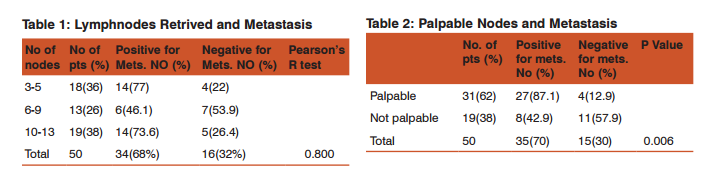
RESULTS Between August 2007 to August 2007, 50 patients presented with breast cancer and underwent surgery were analysed. The mean ages of the patients were 48 years (range 19- 85 years) and maximum occurrence was in the age group above 50 yrs (48 %). All the patients presented with lump in the breast and out of 50 patients in 32 (62 %) ipsilateral lymph nodes were clinically palpable and in 19 (38 %) not palpable. Modified radical mastectomy was performed in 35 (70%) and total mastectomy in 15 (30%) patients, and axillary clearance up to level II in all the patients. The number of lymph nodes retrieved varied from 3 to 13, 3 – 5 in 18(36%), 6-9 in 13 (26%) and > 10 in 19 (38%) patients. Histopathological examination showed infiltrating Ductal carcinoma in 46 (92 %) and intraductal carcinoma in 2 (4%), medullary in 1(2%), lobular in 1(2%). Table 1 compares the number of nodes retrieved with metastatic node and Pearson’s R test did not show any statistical significance. Among the clinically palpable axillary lymph node patients (31) in 27 (87%) patients the lymph nodes were histopathologically positive and in 4 (12.9 %) patients nodes were negative and these findings were statistically significant (p value 0.006). Table 2
DISCUSSION Axillary lymph node status is one of the most important prognostic factor and influences treatment policy in breast cancer. ALND offers excellent loco regional control and improves overall survival 1 . It has been reported that clinical examination of the axillary region is falsely positive in up to 30 percent of cases, and about 30 percent with clinically negative have node involvement on axillary dissection 2 . Node positivity is influenced by the number of nodes retrieved and this depends on the extent of axillary clearance, nodes exceeding ten to have a higher probability of metastasis 5 .In this study only in 38 percent of patients had ten or more retrieved, because our dissection is limited to level II only. Patients with palpable axillary nodes may elect to proceed to axillary clearance since the probability of axillary node involvement is high. The potential complications and the doubtful benefit of ALND have led to the methods of pre operative diagnosis of involvement of axillary nodes. Ultrasound guided fine needle aspiration or core needle biopsy of axillary node is positive only in 41 percent of patients 3 .
Sentinel lymph node biopsy (SLNB) is emerging as an alternative to diagnose axillary node metastasis and to avoid an ALND in node negative patients. Though early results are promising still this technique needs validation. In a recent study by Specht et al have questioned whether SLNB should be considered in breast cancer patients with palpable Axillary lymph node and inconclusive ultrasound guided FNAC or core needle biopsy 6 . According to Axelson et al, SLNB is acceptable in patients with T1-2 and clinically node negative breast cancer 7 . Lymen G.H. et al have recommended ALND in clinically palpable axillary lymph node irrespective of SLNB result and in SLNB positive patients to undergo minimum level II clearance 4 . Large primary tumours have higher rate of Axillary lymph node metastasis but lymphatic infiltration causes decreased identification rate and increased false negative rate in SLNB 8 . According to Parmar V et al axillary sampling is a better alternative to SNB in operable breast cancer 9 . Forrest has stated that axillary sampling helps to identify a node positive axillary region and to select patients for radiotherapy 10. A study on sampling of axillary lymph node in UK has shown that the higher lumber of nodes harvested, higher numbers of metastatic nodes identified. In this study median number of nodes retrieved were 8 (range 0-30) 11. Alternative to axillary sampling up to 30 nodes followed by radiotherapy, prophylactic axillary clearance is a better option for operable breast cancer with clinically palpable lymph nodes 12. In this study, significant number of nodes showed metastasis in clinically palpable axillary lymph nodes. According to Boon et al, in clinically palpable axillary node patients axillary dissection is of therapeutic value and has this advantage over radiotherapy 13. A Meta analysis of six trials including 3000 revealed a survival benefit of 5.4 percent who underwent prophylactic ALND 14.
CONCLUSION Axillary lymph node status remains as one of the most important prognostic factor and it is difficult to confirm metastasis in axillary lymph node irrespective of pre operative US guided FNAC or true cut biopsy or Sentinel lymph node biopsy. Present study has shown Routine Axillary Lymph node dissection (ALND) in clinically palpable axillary lymph node removal has therapeutic value and confirms metastasis and helps in further management. However, further study with larger number of patients is necessary to confirm.
ACKNOWLEDGEMENT: Authors duly thank the department of general surgery, Mahatma Gandhi Medical College and Research institute and Sri Balaji Vidyapeeth University, for permitting us to publish the dissertation as an article in IJCRR. Authors also acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Conflict of interest: All authors declare that there is no conflict of interest.
References:
1. Beenken SW, Urist MM, Zhang Y, Desmond R, Krontiras H, Medina H, et al. Axillary lymph node status, but not tumour size, predicts loco-regional recurrence and overall survival after mastectomy for breast cancer Ann.Surg. 2003;237:732-8
2. Sacks NPM, Baum M: Primary management of carcinoma breast Lancet 1993; 342:1402-1408
3. Deurloo EE, Tanis PJ, Gilhuijs KG. Muller SH, Kröger R, Peterse JL, Rutgers EJ, et al. Reduction in the number of sentinel lymph node procedure by preoperative ultrasonography of the axilla in breast cancer, Eur J cancer 2003;39(8):1068-73.
4. Lyman G.H, Giuliano AE, Somerfield MR, Benson AB, Bodurka DC, Burstein HJ et al. American Society of Clinical Oncology guideline recommendations for sentinel lymph node biopsy is early-stage breast cancer J.Chin oncol 2005;23(30):7703-20.
5. Fisher B, Wolmark N, Bauer M et al, The accuracy of clinical nodal staging and of limited axillary dissection as a determinant of histologic nodal status in carcinoma of breast. Sur Gynaec OBst 1981; 152 (6):765-72.
6. Specht Mc, Fey JV, Borgen PL, Naik AM et al. Is the clinically positive axilla in breast cancer really a contra indication to sentinel lymph node biopsy? J. Am. Coll. Surg. 2005; 200(1):10-14.
7. Axelsion CK, Rank F, Blicher Toft M, Mouriden HT, Jenson MB, Impact of axillary dissection on staging and regional centre in breast tumours < 10mm –The Danish breast cancer Cooperative Group (DBCG) Rigshsontalet, Copenhagen, Denmark Acta Oncol 2000;39:283-9.
8. Samphao S, Eremin JM, El-Sheemy M. Rodier JF, Velten M, Wilt M et al. Management of the axilla in women with breast cancer, current clinical practice and a new selective targeted approach. Ann Surg. Onco 2008; 15 (5):1282-96.
9. Parmar V, Badwe R, Tuttra I, Chinoy R, Hawaldav R. Sentinel node biopsy in operable breast cancer. Ind J Surg. 2003; 65:361- 365.
10. Forrest AP, Everington D, Mc Donald CC, Steele RJ, Chetty U, Steward HJ, The Edinburgh randomized trial of axillary sampling or clearness after mastectomy, Br. J. Surg. 1995;82:1504- 8.
11. Kutiyanawala MA, Sayed M, Scotter A, Windle R, Rew D. Staging the axilla in breast cancer and audit of lymph node retrieval in an UK regional centre. EUR J Surg Oncol 1998;24:280-2
12. NIH consensus conference. Treatment of early stage breast cancer. JAMA ; 1991:265(3):391-5
13. Boon, Owen U, Richard T, John B. Frequency and predictors of axillary lymph node metastasis in invasive breast cancer. ANZJ Surg. 2001; 71:723-728.
14. Orr R K, The impact of prophylactic axillary node dissection on breast cancer survival – a Bayesian Meta analysis. Ann Surg. Oncol 1999; 6(1):109-16.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





