IJCRR - 10(5), March, 2018
Pages: 23-29
Date of Publication: 15-Mar-2018
Print Article
Download XML Download PDF
Investigation of the Efficiency of Endotracheal Aspiration by Sheep Lung Modeling: Experimental Study
Author: Faruk Cicekci, Ata Ozturk, Inci Kara
Category: Healthcare
Abstract:Background: The clinical and radiological evaluation of endotracheal suctioning (ETS), which is performed as a blind procedure has incapacities. The purpose of this study was to indicate that angulation of the ETT tube tip to both lung sides is an important factor in the progression and orientation of the ETSC in the bronchial system.
Method: The five sheep lung was dissected to reveal bronchial system. anesthesiologist inserted the catheter into the endotracheal tube at neutral tube tip position. Then tube tip was rotated 30º and 45º to the right and 30º and 45º to the left respectively. The advancement and orientation of ETSC in the tracheobronchial system were dynamically observed with 625 insertion done by 5 different anesthesiologists.
Results: The sheep tracheobronchial system can be used as a model in morphological studies. The known access limitations of an ETSC were documented in the animal model by dynamically observing the advancement and orientation of an ETSC.
Conclusion: It can be entered both bronchial systems by obtaining a least 30\? of angle to ETT tip position towards each lung side.
Keywords: Sheep lung modelling, Endotracheal suctioning catheter, Selective endotracheal suctioning, Intubation tube position
DOI: 10.7324/IJCRR.2018.1054
Full Text:
INTRODUCTION
Endotracheal suctioning (ETS) is one of the most common supporting prevention in intensive care units (ICU) to suction overage respiratory secretions and improve respiratory function 1,2. The “blind” nature of advancing the suction catheter may be one of the major limitations to the procedure, and may lead to less efficient suctioning. However, failure to aspirate both sides of the bronchial system can have numerous detrimental effects 2-4. The effectiveness of tracheal suctioning is directly proportional to the advance and orientation of the suction catheter to both sides of the tracheobronchial tree and the vacuum characteristics 1. Although generally single-sided suctioning is performed in ETSC, practitioners believe that they have completely performed the procedure because they do not take into consideration the complex morphological characteristics of the bronchial system. Connection of the developed complications to nonstandard techniques or causes such as removing from the ventilator rather than single-sided suctioning results in delays in diagnosis and interventions 1-5. In order for ETSC to be effective, it constitutes a necessity to enter the right and left bronchial system. Since the control of ETSC through imaging techniques is not possible for every patient, it is necessary to determine the effectiveness of the procedure on a model consistent with the human.
Therefore, this study aimed to indicate that angulation of the ETT tube tip to both lung sides is an important factor in the progression and orientation of the ETSC in the bronchial system.
MATERIALS AND METHODS
The study protocol was reviewed and approved by the ethical review board of Selcuk University, Veterany Medicine (Ref No:2015-06-29). Sheep lung were supplied from Konya municipality slaughterhouse a day before experiment.
The five sheep lung was dissected to reveal bronchial system. Bronchial tissue, 2x1 cm from the carina and 1x1 cm from the bronchial branching areas was removed to open windows to observe the movement of the ETSC (Fig 1). The sheep lung was placed on the table so that the membranous part of the trachea faced the dorsal. The trachea was intubated by using a size 8.5 endotracheal tube (B?çakç?lar I.D 8.5, Istanbul, Turkey) so that the tip of the tube was 1 cm above the carina and the cuff was inflated with 20 cm water pressure. In order to indicate the orientation, the blue line on the endotracheal tube was fixed precisely on the middle anterior-posterior line of the trachea. This position was designated the neutral position. An aspiration catheter (B?çakç?lar 16 Ch, Istanbul, Turkey) was used for ETS. Primarily, anesthesiologist inserted the catheter into the endotracheal tube at neutral tube tip position. Then tube tip was rotated 30º and 45º to the right and 30º and 45º to the left respectively. Each anesthesiologist inserted the catheter five times for each tube tip position for each sheep lung. Each anesthesiologist conducted 25 insertion on each of the five lungs. Thus a total of 625 insertion were performed on five different sheep lung. The side (left or right sheep lung) and the final point that the catheter reached were noted.
The data were loaded on Statistical Package for Social Science (SPSS, 20.0 SPSS FW, SPSS Inc., Chicago, IL., USA), which assessed the frequencies and percentages of categorical variables.
RESULTS
After rotation of ET left (30°- 45°) or right (30°- 45°) the intubation tube tip faces to lateral walls of trachea instead ventral. This leads the first contact of ETSC after ET tip to lateral wall rather than medial wall of any main bronchus as in neutral position. After initial contact, catheter advancement was similar as in neutral position. In either rotation, the ultimate point of advancement were the relevant dorsal basal segment of the diaphragmatic lobe.
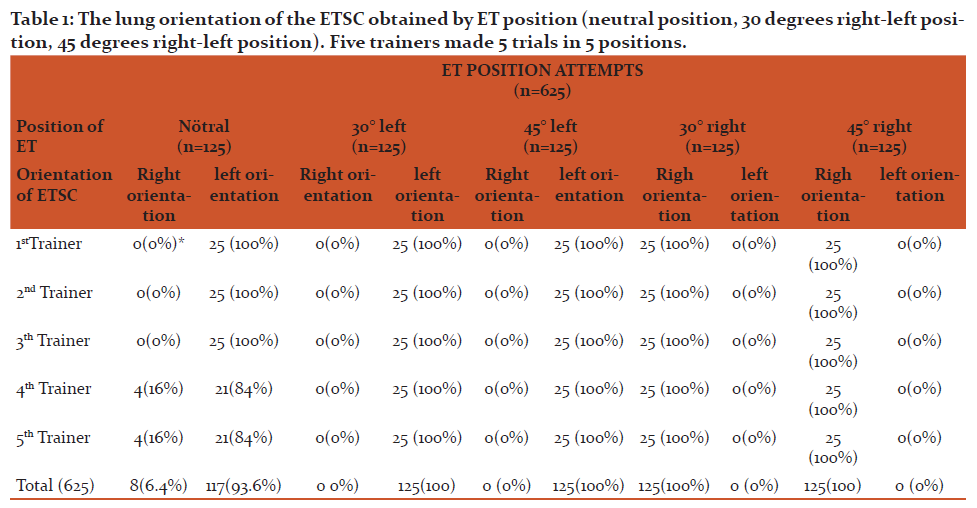
A total of 625 insertions were conducted. At neutral position of ET, the catheter was entered to the left in 117 (93.6%) insertions and to the right in 8 (6.4%) insertions. In neutral position, unlike other anesthesiologists, the anesthesiologists 4 and 5 entered to the right in lung 2 and 3.The ETSC was oriented left bronchial tree (100%) in all left oriented positions of ET (30º or 45º). Similarly the ETSC was oriented right bronchial tree (100%) in all right oriented positions of ET (Table 1).
DISCUSSION
The primary objective of this investigation was to evaluate the ETSC advancement and orientation in the tracheobronchial tree and the factors responsible for differences.
Considering that it is necessary to enter and clean each lobe bronchus for the effective aspiration6,7, it should be presented how successfully this can be performed through current aspiration techniques.
Detecting the access limitations of ETSC on the patient brings along a number of difficulties. It is almost impossible to check through radiological examinations performed during the procedure whether both bronchial systems are accessed for an effective ETSC5. In conventional radiological studies that constitute the basis of control, the image is masked by lung parenchyma. Right and left main bronchus can be viewed up to 3-4 cm after the carina and then the image gets lost inside lung parenchyma. Another disadvantage of conventional imaging is that it is two dimensional and does not provide any information regarding the position of ETSC in the lumen. In this case, the position of ETSC and its relationship with the lobar bronchial orifices opening to the main bronchi cannot be determined although they are on the same plane. Pathological appearances that are frequently observed in intensive care patients such as atelectasis, pleurisy and infiltration make the radiological follow-up of ETSC much more complicated.
According to observations on sheep model, the access limitations of an ETSC can be divided into three problematic areas. These are the space distal to the intubation tube cuff, the bronchial system that cannot be accessed and the bronchi that cannot be aspirated in the successfully accessed bronchial system.
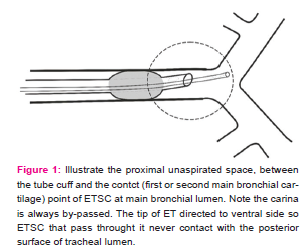
The space between the tube cuff and the contact point of ETSC at right or left main bronchial lumen is the most proximal problematic area. The main source of the secretions that accumulate around the cuff is the bronchial system that cannot be accessed. In addition, the late aspiration of the accessed side also contributes to the accumulation of secretions. ETSC is suspended between the tip of intubation tube and the point where contact with bronchial wall. The carina is bypassed in almost all cases. This means not only the cuff region but the carina and most proximal part of (first cm) of main bronchi are not aspirated. This differs from the orientation that occurs after contacting the carina in the case of foreign-body aspiration 8.Then catheter is directed from medial to posterior aspect of bronchial lumen in the few millimetres of advancement where the effective aspiration come on because the secretions accumulate on posterior surface of bronchial lumen because of gravity (Fig 1).
While one of the lungs is aspirated, only rarely can the other lung be aspirated with the current form of ETS. Right is dominant side in ETSC advancement in human lung (80-92%). Therefore, advancing ETSC into the left is difficult (8-20%), which means that one side cannot be aspirated easily 2,3,5,9,10. Even in cases performed by experienced practitioners, with the head positioned and a special catheter used, the left bronchial system can be accessed at a rate of 50% 3,5,7,9,11.
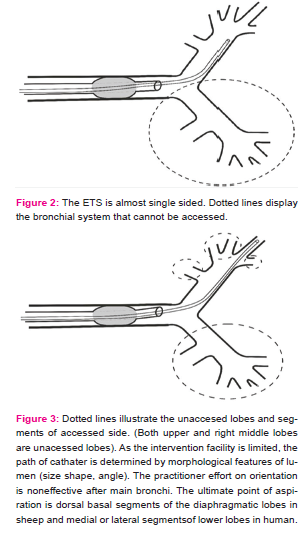
Only bronchoscopy guarantees the aspiration of the tracheobronchial system by entering both sides 5,12. Entering into the left bronchial system does not guarantee successful entry into the right bronchial system in the same session, which means that the bronchial system is usually aspirated in one side only during ETS. In our study, it was achieved a rate of 86% dominancy on one side in neutral position, which is close to the rate of 80 – 92% stated for humans in the previous studies (Fig 2).
The blind nature of procedure and the estimation that the main bronchi is reservoir of accumulated secretions result in whether lobe bronchi were reached during ETS was left out of the clinical evaluation. The drainage of both upper lobes and the right middle lobe while the patient is in a supine position, without any problems in most cases, has made the clinical examination of these lobes unnecessary. In this study, the catheters reached the diaphragmatic lobe bronchi in the sheep lungs, which are considered the equivalent of the lower lobes in humans, in all of the experiments (100%). However, the apical, cardiac intermediate and apico-cardiac lobes in sheep could not be accessed in any of the insertions (0%), which supports the idea that the right upper, middle and left upper lobes in humans cannot be accessed with the ETSC (Fig 3).
The factors that affect the access facility of an ETSC can be grouped into four main categories. These are endotracheal tube tip position, morphological structure of the tracheobronchial system, factors related to the practitioner and the material characteristics of the catheter.
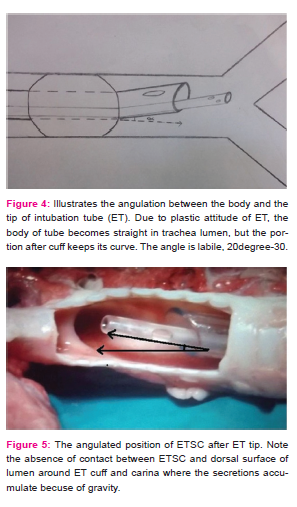
First of all, intubation tube tip position was not evaluated as a factor but it is stated that the orientation of the ETSC progressed depending on the angulation of the carina. During the observations through the windows opened to the tracheobronchial system, the intubation tube tip angulated toward the ventral side of the trachea. This situation results from the curved body structure of the intubation tube, which becomes straight in the tracheal lumen and (tip portion after cuff preserve its natural form) then has its tip propped up after the cuff, causing a slight curve toward the ventral side. As ETSC was directed ventrally just after ET tip, the accumulated secretions on dorsal surface of lumen around ET cuff and carina was impossible (Fig 4,5,6).
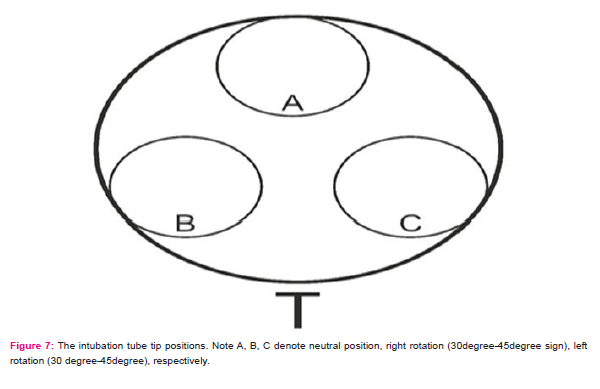
Since the ET tip ended in angulated manner after cuff, the rotational movement of ET changes the position of ET tip13. After rotation of ET to left (30°-45°) or right (30°-45°) the intubation tube tip faces to lateral walls of trachea instead ventral (Fig 7). This leads the first contact of ETSC to lateral wall rather than medial wall of any main bronchus. In real situation deviation of ET from neutral position is not uncommon14. Minor position changes such as fixing of ET to left or right side of mount, the stirring of patient head, the burden of auxillary pipes on ET are few of agent that may facilitate the change of neutral position of ET and may lead inevitable effects on ETSC orientation13,15,16. The access rates of 30o and 45o rotation to left and right displays in Table 2. The entrance rates at 30o and 45o for oriented side were %100. Both bronchial systems can be accessed by rotation of ET even 30o to left or right. Considering that it is stated in the previous studies that access to the left occurs at rates between 8–15% with the aspirations performed by conventional methods, our method (rotation of tube at 30o or 45o) which provides full access to both systems, will prove to be highly useful.
Although there is no intervention facility for ETSC after ET, the path of ETSC is determined by morphologic features of tracheobronchial tree (as latter mention practioners factor can effect just before first contact).The morphology of the tracheobronchial system in the study implies lumen dimensions, lobar bronchial orifice position and as well as their angles17,18. ETSC movement will continue until the lumen dimension becomes equal to or smaller than the catheter size. It was observed that lumen dimensions in the study did not have any effect on the catheter movement.
Solid objects, such as a catheter, resist to change their shapes and move in the direction of the applied force. The main axis in the bronchial system is the plane that the right of left main bronchi constitutes extending from the proximal to the distal. Due to its material characteristics (hardness and stiffness) and absence of guiding mechanism, an ETSC cannot advance at right or near-right angles19. Unreasonable efforts result in bending and kinking of the catheter20. In the study, the ETSC could not access the apical, cardiac intermediate and apico-cardiac lobes in sheep due to their right angle to the right and left main bronchial system (0%). Right upper and middle lobes and left upper lobes in humans, which are considered to be the equivalent of the aforementioned sheep lobes, also intersect at which shows a similar angulation an angle of approximately 90° to the main bronchus, making catheter access impossible.
The ultimate point of that the ETSC reaches in the bronchial system is the dorsal basal segment of the diaphragmatic lobes in sheep (100%). This is consistent with the morphologic features mentioned above. Taking into account of sheep model, the ultimate point of advancement in human will be medial or posterior segments of the lower lobes.
Four out of five lobes in single-sided ETS and three out of five lobes in bilateral ETS cannot be aspirated because of the difficulties presented above. Considering that it is necessary to aspirate all the lobes for effective aspiration, it can be concluded that effective aspiration cannot be performed even with bilateral ETS.
Although access to the left bronchial system at neutral position was dominant in the study (93.6%), some anesthesiologists (6.4%) entered the right bronchial system. We postulate that personal factors caused experimenters 4 and 5 to enter the right bronchial system in all experiments on lungs 2 and 3 at neutral position; these personal factors include which hand they used, catheter pushing speed, manoeuvres to the right or left while pushing and other skills they gained before hand. Regardless, the fact that all anesthesiologists consistently accessed the same side in all tube positions supports our assertion.
The AARC report21 mentions scarcely on aspiration competence. The rational of the report is at functional manner that satisfactory aspiration means sufficient oxygenation of blood. The estimation is based on two consideration; the ciliary motion can afford to carry the secretions of even the most distal parts of bronchial system to proximal and just after the tip of ET, the ETSC contacts with secretions and aspiration takes place22,23. Contary to assertions in AARC, the experiment revealed the central regions such as carina and cuff periphery was not aspirated.
AARC recommends swallow aspiration because of less traumatic potential than deep aspiration21 but neither technique is superior for removing secretions. The secretions of unaspirated side inevitably accumulate and may result in devastating complications1. The current guidance on endotracheal suctioning may need to be investigated the optimal methods to aspirate more central parts of tracheobronchial tree such as mucus slurper24, mucus shaver 25 or modification of ET tip confugration to maintain contact just after ET tip rather than to major on present tecniques and strategies.
The scope of the modelling focused on the first two factors; the tube tip position and morphological structure of the tracheobronchial system. The third and fourth factors, based on the practitioner and the physical and material characteristics of the catheter, were not included in this study. Further studies could be designed for evaluating the effects of these factors.
CONCLUSION
In our study, by using a sheep lung model, we endeavoured to show that the ETSC was not located sufficiently. We believe this is because the tracheobronchial system anatomy are not well understood and catheter movement cannot be foreseen by most clinicians26. The influence of the intubation tube tip position and practitioner factors on the effectiveness of ETS are points that have not been discussed in the previous studies properly. Direct observation of the procedure on a dynamic model will help to identify previously ignored factors in clinical and radiological evaluations. The fact that ETSC does not have a guidance mechanism causes ET tip position to become the main determinants in guiding the ETSC. Therefore, we consider that it can be entered both bronchial systems by obtaining a 30° of angle towards each side.
The authors role and responsibilities:
F.C: Data collection, study design, literature search, analysis of data, review of manuscript
A.A.O: Study design, manuscript preperation, review of manuscript
I. K: Analysis of data, manuscrits preperation,review of manuscripts
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
No conflicts of interest declared.
There was no financial support for the study. The expenditures were paid by the contributers of manuscripts.
The authors of manuscripts certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.

References:
- Sallum Zeitoun S, Lucia Botura A, Diccini S. A prospective, Randomized study of ventilator-associated pneumonia in patients using a closed vs. open suction system. J Clin Nurs 2003;12:484-9.
- Siempos II, Vardakas KZ, Falagas ME. Closed tracheal suction system for prevention of ventilator-associated pneumonia. Br J Anaesth 2008;100:299-306.
- Anthony JS, Sieniewicz DJ. Suctioning of the left bronchial tree in critically ill patients. Crit Care Med. 1977;5(3):161-2.
- Lv J, Wu J, Guo R, Liu X, Yan B, Deng H. Laboratory test of a visual sputum suctioning system. Respir Care 2013;58(10):1637-1642.
- Panacek E A, Albertson T E, Rutherford W F, Fisher C J, Foulke G E. Selective left endobronchial suctioning in the intubated patient. Chest. 1989;95(4):885-7.
- Matsuoka H, Nakamura H, Nishio W, Sakamoto T, Harada H, Tsubota N. Division of the pulmonary ligament after upper lobectomy is less effective for the obliteration of dead space than leaving it intact. Surg Today 2004;34:498–500.
- Haberman PB, Green JP, Archibald C, Dunn DL, Sheldon R. Hurwitz, Ashburn WL, Moser KM. Determinants of successful selective tracheobronchial suctioning. N Engl J Med 1973; 289:1060-3.
- Cotton RT, Rutter MJ: Foreign body aspiration. In: Chernick V, Boat TF, Wilmott RW, Bush A (eds.), Kendig’s disorders of the respiratory tract in children. 7th edn. Elsevier Saunders, Philadelphia, 2006;610–5.
- Kubota Y, Magaribuchi T, Ohara M, Fujita M, Toyoda Y, Asada A, Harioka T. Evaluation of selective bronchial suctioning in the adult. Crit Care Med. 1980;8(12):748-
- Hart TP, Mahutte CK. Evaluation of a closed-system, directional-tip suction catheter. Respir Care. 1992;37(11):1260-5.
- Freedman AP, Goodman L. Suctioning the left bronchial tree in the intubated adult. Crit Care Med. 1982;10(1):43-5.
- Jung RC, Gottlieb LS. Comparison of tracheobronchial suction catheters in humans. Visualization by fiberoptic bronchoscopy. Chest. 1976 Feb;69(2):179-81.
- Tripathi M, Arora M. Evaluation of a simple technique for rapid access to left main bronchus. J Indian Med Assoc. 1996;94(12):447-8.
- Weiss M, Knirsch W, Kretschmar O, Dullenkopf A, Tomaske M, Balmer C, Stutz K, Gerber AC, Berger F. Tracheal tube-tip displacement in children during head-neck movement--a radiological assessment. Br J Anaesth. 2006;96(4):486-91.
- Conrardy PA, Goodman LR, Lainge F, Singer MM. Alteration of endotracheal tube position. Flexion and extension of the neck. Crit Care Med. 1976;4(1):8-12.
- Donn SM, Kuhns LR. Mechanism of endotracheal tube movement with change of head position in the neonate. Pediatr Radiol. 1980;9(1):37-40.
- Harjeet, Sahni D, Batra YK, Rajeev S Anatomical dimensions of trachea, main bronchi, subcarinal and bronchial angles in fetuses measured ex vivo. Paediatr Anaesth. 2008;18(11):1029-34.
- Daroszewski M, Szpinda M, Flisi?ski P, Szpinda A, Wo?niak A, Kosi?ski A, Grzybiak M, Mila-Kierzenkowska. Tracheo-bronchial angles in the human fetus - an anatomical, digital, and statistical study. Med Sci Monit Basic Res. 2013;16(19):194-200.
- Ceschinski H, Henkes H, Weinert HC, Weber W, Kühne D, Monstadt H. Torquability of microcatheter guidewires: the resulting torsional moment. Biomed Mater Eng.2000;10(1):31-42.
- Scott AA, Sandham G, Rebuck AS. Selective tracheobronchial aspiration. Thorax. 1977;32(3):346-8.
- Restrepo RD, Brown JM, Hughes JM. AARC Clinical Practice Guidelines. Endotracheal suctioning of mechanically ventilated patients with artificial airways 2010. Respir Care 2010;55(6):758-64.
- Rubin BK. Physiology of airway mucus clearance. Respir Care. 2002;47(7):761-8.
- Ficker JH. Physiology and pathophysiology of bronchial secretion. Pneumologie. 2008;62 (1):11-3.
- Kolobow T, Li Bassi G, Curto F, Zanella A. The Mucus Slurper: A novel trachealtube that requires no tracheal tube suctioning. A preliminary report. Intensive Care Med. 2006;32(9):1414-8.
- Berra L, Coppadoro A, Bittner EA, Kolobow T, Laquerriere P, Pohlmann JR, Bramati S, Moss J, Pesenti A. A clinical assessment of the Mucus Shaver: a device to keep the endotracheal tube free from secretions. Crit Care Med. 2012;40(1):119-24.
- Ho?ten T, Topçu S. The importance of bronchoscopic anatomy for anesthesiologists. Tuberk Toraks. 2011;59(4):416- Review
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





