IJCRR - 3(11), November, 2011
Pages: 179-183
Print Article
Download XML Download PDF
COMPARISION OF LOCKING PLATE AND CONVENTIONAL PLATE IN TREATMENT OF MANDIBULAR FRACTURE
Author: Bindu Ramesh, S M Kotrashetti, Umashankar G K, Ramesh B H
Category: Healthcare
Abstract:The purpose of this study was to compare the clinical outcome and complications between the
2.0mm locking titanium miniplate and 2.0mm conventional titanium miniplate in the treatment
of mandibular fractures. 20 cases were selected for the study. 10 cases were treated using
locking plates and 10 cases were treated using conventional plates. Clinically and radio
graphically both the groups were followed up for healing and complications. There were a few
complications in both the groups. There was a case of infection in group treated with 2.0mm
locking titanium miniplates and a case of malocclusion and a case of mobility in group treated
with conventional titanium miniplates. Our results show no significant difference in the
treatment outcome between locking plates and conventional plates.
Keywords: mandible fracture, locking plate, infection, malocclusion, mobility
Full Text:
INTRODUCTION
Treatment of mandibular fractures has evolved over the past decades from supportive bandages, splints, circummandibular wiring, extra oral pins, and semi rigid fixation with transosseous wiring to rigid fixation with compression plates and more lately, semi rigid fixation with non compression miniplates1-8 . Raveh et al developed locking plate and screw system in the mid 1980s where he incorporated the principles of external fixation device into a bone plate to fix fractures. These plates achieve stability by locking the screw to the plate and have shown to enhance the fixation stability9 . The disadvantage of the conventional plate and screw systems is that the plate must be perfectly adapted to the underlying bone to prevent alterations in the alignment of the segments and changes in the occlusal relationship. The locking system was used earlier in reconstruction plates and is now incorporated into the miniplates. A unique advantage to locking screw/plate system is that it becomes unnecessary for the plate to have intimate contact with the underlying bone, making plate adaptation easier. The purpose of this study was to compare the clinical outcome and complications of the two plating systems.
MATERIALS AND METHODS
Study was conducted at KLE‘s Institute of Dental Sciences and Hospital, Belgaum, Karnataka, India from March 2004 to April 2005. Twenty cases reporting to the hospital with mandible fractures were selected. 10 cases were treated using the COMPARISION OF LOCKING PLATE AND CONVENTIONAL PLATE IN TREATMENT OF MANDIBULAR FRACTURE Bindu Ramesh1 , S M Kotrashetti2 , Umashankar G K3 , Ramesh B H4 1 Department of Oral and Maxillofacial surgery, M R Ambedkar Dental College Bangalore 2Department of Oral and Maxillofacial Surgery, KLE‘s Institute of Dental Sciences Belgaum 3Department of Community Dentistry R Ambedkar Dental College, Bangalore 4Department of Pathology, Raichur Medical College, Raichur E-mail of Corresponding Author: binduramesh80@yahoo.com 180 International Journal of Current Research and Review www.ijcrr.com Vol. 03 issue 11 November 2011 conventional titanium miniplates and 10 cases were treated using 2.0mm conventional titanium miniplates.The diameter of the screws used was 2mm in diameter and 8mm in length. The quality of titanium used was DSTM-B grade 1. The composition of which as per the guidelines of Non Ferrous Metal Technology Development Corporation (N.F.T.D.C) Kanchanbhag, Hyderabad.
Criteria for patient selection was
- Patients who were available for follow up
- Fractures requiring or indicative of open reduction
- Fractures of mandible except condyle
- No other facial fractures
- Patients without medical illness All patients were evaluated for adverse habits, location and type of fracture, number of fracture, time from injury to presentation, operating time immediate and late post operative complications. All the patients were followed up for a period of 3 months to evaluate healing or to check for complications. Surgical technique used to place the plate was same for both the plates except that the locking plates required a drill guide to place the screw perpendicular to the plate.
All the patients were placed on IMF preoperatively with arch bars. In all cases intraoral approach was used except the angle fractures where extra oral approach was used to place the locking plates. All fractures were treated according to Champy‘s line of osteosynthesis. Two plates were placed in fractures involving parasymphysis and symphysis region and single plates were placed in body, angle and the ramus region. All patients were operated under general anaesthesia. Time taken to complete the surgical procedure was recorded in each case. Immediate post operative radiograph was taken to evaluate reduction. None of the patients were placed on IMF post operatively and all the patients were instructed to be on soft diet for the first fifteen post operative days. Patients were recalled for follow up weekly for first one month and then recalled monthly for next two months. At the end of three months radiograph was taken to evaluate the healing and complications. The descriptive measures were used to analyse the data, quantitative values were expressed in percentages and quantitative values were expressed using mean and standard deviation.
RESULTS
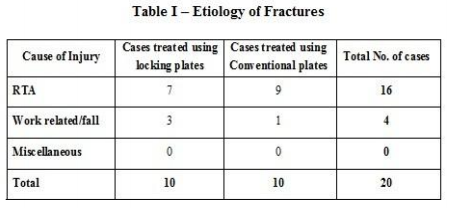
20 patients who met the inclusion criteria were included in the study. There were 18 males and 2 females in the study. A total of 27 fractures were present in 20 cases .14 fractures were present in 10 cases treated using locking titanium miniplate and 13 fractures were present in 10 cases treated using conventional titanium miniplate. The average age was 35±11.07 with a range of 20 to 55 years. The aetiology of trauma was RTA in 16 patients and fall in 4 patients (Table I). The average number of days following trauma was 1 to 8 days (mean 1.8±1.7). Of all the mandible fractures treated with conventional plates and locking plates three developed complications with an overall complication rate of 11.11 %.( Table 2) In the group treated with locking titanium miniplates one fracture developed infection which was treated with plate removal and antibiotics. In group treated with conventional titanium miniplates, one case of mobility and one case of malocclusion was seen. Mobility occurred due to non compliance of patient to post operative 181 International Journal of Current Research and Review www.ijcrr.com Vol. 03 issue 11 November 2011 instruction of being on soft diet for the first 15 post operative days. Mobility was managed using IMF for two weeks and malocclusion was treated by placing the patient on elastics for a week. On comparing the data of results of patients with complications and patients without complications, the average number of days from injury to treatment was more in patients with complications (4.5 days) than in those without complications (3 days). The average age in the group with complications (35.6) and those without complications (35.3) is similar. The average operating time in group with complications is 82.5 min and group without complications is 82.5min. The above mentioned results show no significant difference between the two plating systems and the group with complications and group without complications.
DISCUSSION
The stability of conventional plating system is achieved when the head of the screw compresses the fixation plate to the bone as the screw is tightened. Invariably, overtime, the cortex of the bone adjacent to the plate will resorb. Under ideal conditions the system will remain stable till the fracture has healed, if the plate is not contoured precisely and is not in intimate contact with the bone or if the host is compromised (medically or nutritionally), the ?race? between fracture healing and cortex resorption will be lost and will result in unstable fixation . The locking system will circumvent the need for precise plate adaptation and compensate for host compromise during healing 10, 11. 2.0mm locking plate were first used by Edward Ellis and John Graham in 2002 for treatment of mandible fractures; they found the use of locking plates to be simple and stable 12. On testing the locking plates biomechanically for stability it was shown that these plates are more stable compared to the standard plates13. An in vitro study compared the failure strength of locking plates over conventional plates which showed that the degree of failure are more likely related to bone quality and surgical technique when using 2.0mm plates 14 . Two studies comparing the locking plate and conventional plates have showed that both the plates present similar short term complications 15 . The disadvantage of these plates is that it requires centring the drill hole with the plate hole for locking the screw head into the plate and cost of these plates is more compared to the conventional plate.
Overall complication rate in group using locking plates is 7.14% and the group using conventional plates is 15.38%. Application of statistical analysis for these results is not feasible because of small sample size. On comparing the data of both groups it is found that there is no advantage of one group over the other, hence the choice of plate depends on the ease of placement and the cost of one plate over the other.
CONCLUSION
Mandible fractures have different treatment modalities, the one which is most commonly used clinically are the miniplates. Locking plate is a modification of the conventional miniplates which offers certain advantages over the conventional plates. This study shows that practically conventional plates and the locking plates have similar complications and there is no advantage of one plate over the other

References:
1. Fonseca Raymond J ?Oral and Maxillofacial Trauma? Pennsylvania, 182 International Journal of Current Research and Review www.ijcrr.com Vol. 03 issue 11 November 2011 WB Saunders Company,2nd Edition, vol 1, 359-414, 1991.
2. Edward Ellis III: Rigid skeletal fixation of a fracture. J. Oral Maxillofacial Surg 51: 163 -173, 1993.
3. Gyorgy Szabo, Adam Kovacs, Gyorgy Pulay: Champy Plates in Mandibular surgery. Int J Oral Maxillofac Surg 13: 290 – 293, 1984.
4. David Frost, Amir El – Attar, Khursheed F Moos: Evaluation of metacarpal bone plates in the mandibular Fracture. Br J Oral Surg 21: 214 – 221, 1983.
5. Edward Ellis and G E Ghalli : Lag Screw fixation of Mandibular Angle fractures:J Oral Maxillofac Surg 49: 234 – 243, 1991
6. Anna- Lisa Soderholm, Christian Lindquist, Kai Skutnabb, and Berton Rohan: Bridging of mandibular defects with two different reconstruction systems: An experimental study. J Oral Maxillofac Surg 49:1098 – 1105, 1991.
7. Timothy Edwards, David J David: A comparative study of miniplates used in the treatment of mandible fractures. Plast Reconst Surg 97, 1150 – 1157, 1996.
8. Raveh J, Sutter F, and Hellem: Surgical Procedures for reconstruction of lower jaw using the titanium coated hollow screw reconstruction plate system: Bridging of defects. Otolaryngol Clin North Am 20 : 535, 1987
9. Brian Alpert, Ralf Gutwald and R Schmelzeisen: New innovations in craniofacial fixation the 2.0 lock system. Keio J Med 52(2): 120 – 127, June 2003.
10. Richard H Haug, Chad C Street, Michele Goltz: Does plate adaptation affect stability? A biomechanical comparison of locking and non locking plates. J Oral Maxillofac Surg 60: 1319 – 1326, 2002.
11. Edward Ellis III and John Graham: Use of 2.0mm locking plate /screw system for mandibular fracture surgery. J Oral Maxillofac Surg 60: 642-645, 2002.
12. Ralf Gutwald, Brian Alpert and Rainer Schmelzeisen: Principle and stability of locking plates.Keio J Med 1: 21 – 24, March 2003.
13. Collins C P, Pirinjian- Leonard G, Tolas A and Alcalde R: a prospective randomized clinical trial comparing 2.0mm locking plates to 2.0mm standard plates in the treatment of mandible fractures. J Oral Maxillofac Surg. 62: 1392 – 1395, 2004.
14. Chiodo T, Ziccardi V, Janal M and Sabatini C: Failure strength of 2.0 locking versus 2.0 Conventional Synthes mandibular plates: a laboratory Model. J Oral Maxillofac Surg Oct 64(10) 1475 – 1479, 2006.
15. Singh V, Kumar I and Bhagol A: Comparitive evaluation of 2.0mm locking plate system Vs 2.0mm non locking plate system for mandibular fracture, a prospective randomized study. Int J Oral Maxillofac Surg 2010 Dec 29 [ Epub ahead of print
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





