IJCRR - 3(11), November, 2011
Pages: 84-96
Print Article
Download XML Download PDF
EVALUATION OF THE IMPLEMENTATION OF REVISED NATIONAL TUBERCULOSIS CONTROL
PROGRAMME IN THE PRIMARY HEALTH CENTERS
Author: Shivappa Hatnoor, Sangolli H N, Hemagiri.K, Mallapur M.D, VinodKumar C.S
Category: Healthcare
Abstract:Tuberculosis continues to be one of the most important public health problem worldwide. It
infects one third of the world's population at any point of time. There are approximately 9
million new cases of all form of tuberculosis occurring annually and 3 million people die from
it each year. Out of these 95% tuberculosis cases and 98% tuberculosis deaths are contributed
by developing countries.
India accounts for nearly one third of the global burden of tuberculosis. Around 2.0 million
people are diagnosed to be suffering from tuberculosis every year.1 Tuberculosis kills more
adults in India than any other infectious diseases. More than 1000 people a day i.e one every
minutes die of tuberculosis. Evaluation of the implementation of Revised National Tuberculosis
Control Programme in the three Primary Health Centres of Belgaum District.
A Longitudinal study, data collected by personal interview in the field, all cases diagnosed for
tuberculosis by the Medical Officers of three Primary Health Centers from November 1st 2004
to April 30th 2005.
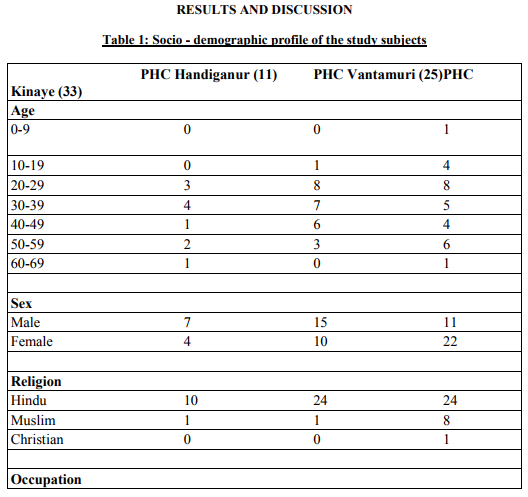
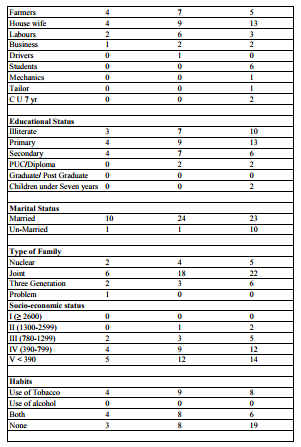
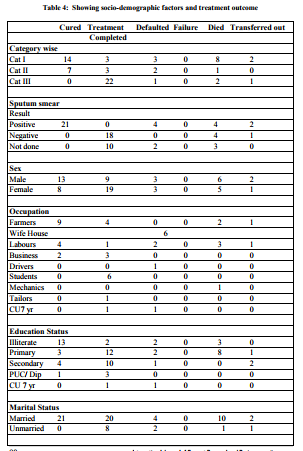
In the present study 48% were males, 52% were females, more than 50% of patients were in the
age group of 20-39 years and majority were Hindus(84%). majority of patients were
Housewives i.e.37.7% followed by farmers i.e. 23.2% and labours 16%. Out of these 69 cases
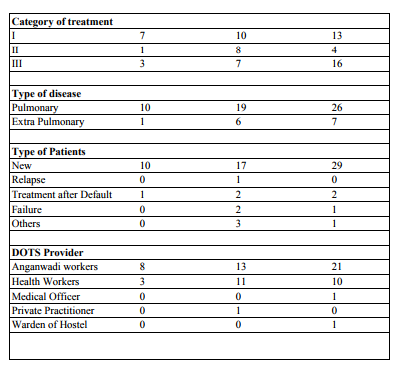
43.5% belonged to category I, 18.8% category II and 37.7% category III. The overall average
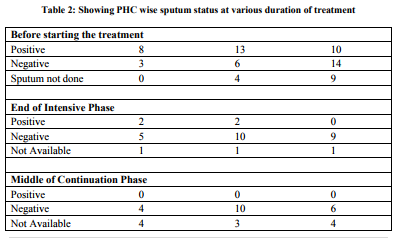
sputum referral in six months was 3.8% and positivity was 11.5%. At the end of Intensive
phase out of 31 sputum positive patients, 77% showed sputum conversion to negativity, 13%
remained positive and 18% were not available for sputum examination. At the end of
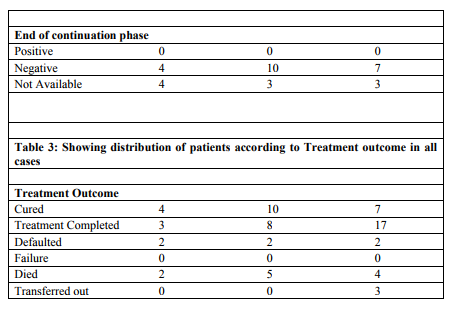
continuation phase whose sputum was positive initially 68% were sputum negative and 32%
were not available. Overall treatment outcome cured were 30.4%, completed the treatment
40.6%, defaulted 8.7%, died 16% and transferred out 4.3%.
Keywords: Tuberculosis, implementation of RNTCP, primary health care
Full Text:
INTRODUCTION
Tuberculosis continues to be one of the most important public health problem worldwide. It infects one third of the world‘s population at any point of time. There are approximately 9 million new cases of all form of tuberculosis occurring annually and 3 million people die from it each year. Out of these 95% tuberculosis cases and 98% tuberculosis deaths are contributed by developing countries (1).
India accounts for nearly one third of the global burden of tuberculosis. Around 2.0 million people are diagnosed to be suffering from tuberculosis every year (1). Tuberculosis kills more adults in India than any other infectious diseases. More than 1000 people a day i.e one every minutes die of tuberculosis(2). Despite the National Tuberculosis Programme since 1992, the desired control of tuberculosis could not be achieved. More over, there has been an increase in the absolute number of tuberculosis patients because of the increase in population. The impending threat of Tuberculosis- HIV co- infection and the emergence of Multi Drug Resistance Tuberculosis have made the situation worse(3). In 1992, an expert committee reviewed the National Tuberculosis Programme and found that less than 30% treatment completion rate, undue emphasis on radiological diagnosis, poor quality of sputum microscopy, multiplicity of treatment regimens, emphasis on case detection rather than on treatment completion, inadequate budgets and shortages of drugs (3). The Revised National Tuberculosis Control Programme introduced in 1993 lays more emphasis on good quality diagnosis by direct sputum smear microscopy and quality drugs, through standardized short course chemotherapy regimens administered under direct observation along with systematic monitoring and evaluation (3). The goal of the Revised National Tuberculosis Control Programme is to cure at least 85% of new sputum smear positive patients detected and to detect at least 70% of all such patients after the goal for cure rate has been met(2). Belgaum district started implementing Revised National Tuberculosis Control Programme from 15th July 2003. K.L.E. Society‘s J.N. Medical College adopted three Primary Health Centres namely Kinaye, Vantmuri and Handignur on 7th April 2004 as such no studies have been done on evaluation of Revised National Tuberculosis Control Programme in these areas. So, this study was taken to evaluate the implementation of Revised National Tuberculosis Control Programme in these areas and also to know the reasons for default of the patients put under Revised National Tuberculosis Control Programme.
OBJECTIVES Evaluation of the implementation of Revised National Tuberculosis Control Programme in the three Primary Health Centres of Belgaum District.
MATERIALS AND METHODS
Study Design: This was a Longitudinal study undertaken to evaluate the Revised National Tuberculosis Control Programme in three Primary Health Centers.
Source of Data: Total population of three Primary Health Centers i.e Kinaye 47,159, Vantamuri 30,756 and Handiganoor 23,452 population.
Inclusion Criteria: All cases diagnosed for tuberculosis by the Medical Officers of three Primary Health Centers from November 1st 2004 to April 30th 2005.
Study Period: From November 1st 2004 to 31st December 2005 (One year One month) Methods
of Data Collection: Using pre-designed and pre-tested proforma the data is collected. The first visit was done when the patient was registered in the Primary Health Center and started on the treatment. The following data
was collected in the first visit Name, Age, Sex, Religion, Occupation, Address, Educational Status, Marital Status, Type of Family, Socio-economic status, DOT provider, Category of Treatment, Disease Classification, Type of patient, result of 1st Sputum (at the start of the treatment) examination and if there are any reasons for initial default. Second visit i.e. First follow-up visit was done at the end of Intensive Phase and the following data was collected regarding the scheduled intake of drugs, result of 1st follow-up sputum examination and about defaulters if any.
Third visit i.e. second follow-up visit was done in the middle of Continuation Phase and the following data was collected regarding the scheduled intake of drugs, result of 2nd follow-up sputum examination and defaulters if any. Fourth visit i.e. third follow-up visit was done at the end of Continuation Phase and the data was collected regarding the scheduled intake of drugs, result of sputum examination at the end of the treatment, about defaulters if any and outcome of the treatment.



References:
1. Kishore J. National Health problem of India 6th edition Century publication New Delhi, 2006. P.No.109-134.
2. A training course Modules 1-4, Managing the Revised National Tuberculosis Programme in your area 4 th printing February 2002 Central Tuberculosis Division DGHS, MOHFW, Nirman Bhavan, New Delhi.
3. Srivastava S.K., Ratan R.K. Srivastava P, and Prasad R: report on Revised National Tuberculosis Control Programme: urban pilot project in Lucknow, Ind J. Tub, 2000,47,159- 162.
4. Chadha S.L. and Bhagi R.P: Treatment outcome in Tuberculosis patients plaud under directly observed treatment short course- A cohort study. Ind.J.Tub,2000,47,155-158.
5. Gupta K.B and Rajesh Gupta; Association between smoking and Tuberculosis Ind. J. Tub, 2003, 50, 5-7.
6. Arora V.K and Rjnish Gupta; Trends of Extra Pulmonary Tuberculosis under Revised National Tuberculosis Control Programme: A study from South Delhi, Ind. J. Tub, 2006, 53, 77-83.
7. Rajasekaran.S, Gunasekaran, H, Jaya Kumar D.D, Jayaganesh.D and Bhanumathi.V; Tuberculosis cervical Lymphadenitis in HIV positive and negative patients Ind .J. Tub, 2001, 48, 201-204.
8. Thomas .A,Chandrasekaran .V, Santha.T,Gopi .P.G, Subramani .R and Narayanan .R.R; sputum examination at two months into continuation phaseHow much does it contribute to define treatment outcome? , Ind. J. Tub, 2006, 53, 37-39
9. Sanjay Rajpal, Dhingra V.K. and Agarwal J.K; Sputum Grading as predictor of treatment outcome in pulmonary tuberculosis; Ind .J. Tub, 2002, 49, 139
10. Sophia Vijay, Balasangameswara V.H, Jagannatha .P.S, Saroja .V.N and Kumar P.Treatment outcome and two half years followup status of new smear positive patients treated under Revised National Tuberculosis Control Programme, Ind.J. Tub, 2004, 51,199- 208.
11. Marina Rajan Joseph, Sunny Orath P, Ea[em C.K; Integrating private Health care in national Tuberculosis Programme: Experience form Ernakulam Kerala, Ind.J. Tub, 2001,48,17-19.
12. Nirupa.C, Sudha.G, Shant.D, Ponnuraja.L, Fatima.R, Chandrasekharan.V, Jaggarajamma .K, Thomas A, Gopi .P.G and Narayanan .P.R; Evaluation of directly observed treatment providers in the Revised National Tuberculosis Control Programme, Ind.J. Tub, 2005,52, 73- 77.
13. Revised National Tuberculosis Control Programme at Glance, central Tuberculosis division Directorate General of Health Services Ministry of Health and Family welfare Nirman Bhavan, New Delhi.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





