IJCRR - 4(8), April, 2012
Pages: 10-15
Date of Publication: 25-Apr-2012
Print Article
Download XML Download PDF
USE OF ANTIMICROBIAL PROPHYLAXIS IN SURGICAL AND MEDICAL INTENSIVE CARE UNITS - A
COMPARATIVE STUDY
Author: Apurva Agrawal, Barna Ganguly
Category: Healthcare
Abstract:Aims: To study the extent and pattern of use of antibiotics for prophylaxis in medical and surgical intensive care units. Subjects and Methods: 100 patients each from SICU and MICU were included inthe study. Case record files were analyzed daily until discharge from ICU or a maximum of 21 days. Details of all antibiotics prescribed for prophylaxis were recorded in a proforma, which were then analyzed using relevant statistical tests. Results: 65% patients in MICU and 99% in SICU received antibiotics (p value < 0.0001). Among patients who received antibiotics, 37% in MICU and 73% in SICU received them for prophylaxis (p value < 0.0001). Average duration of prophylaxis was 2.58 days in MICU and 3.14 days in SICU. 19 (79.14%) patients in MICU and 48 (66.67%) patients in SICU received prophylaxis for more than 24 hours (p value = 0.3690). 15 (62.5%) patients in MICU and 31 (43%) patients in SICU received combination of antibiotics for prophylaxis (p value = 0.156). Third generation cephalosporins were the most commonly prescribed antibiotics for prophylaxis in both ICUs. Conclusion: Widespread use of antimicrobial prophylaxis in ICUs with broad spectrum antibiotics and antibiotic combinations, with duration longer than recommended has emerged as area of concern in present study. Such surveillance studies help in recognition of areas requiring special attention, which can
guide the formulation of antibiotic prescription policies at individual ICU level.
Keywords: Antibiotic, antimicrobial resistance, ICU.
Full Text:
INTRODUCTION
Infections are a frequent problem in Intensive Care Units (ICUs) and thus antibiotics are frequently used. Although antibiotics represent one of the most frequently prescribed classes of drugs among all hospitalized patients, total antibiotic consumption is much higher in the ICU than in general hospital wards. [1] Besides treatment of infections, antibiotics in ICU are administered as prophylaxis to prevent or limit major infections in critically ill patients. [2] Antibiotic prophylaxis is highly effective in some clinical settings, but in others, it accounts for misuses of antimicrobials, and may even be deleterious. [3] A number of studies have justified antibiotic prophylaxis in dirty or contaminated surgical procedures, where the incidence of wound infections is high, but such use must not be extended beyond 24 hours. [3] These include less than 10% of all surgical procedures. In clean surgical procedures, which account for approximately 75% of the total, antibiotics should not be routinely used as the expected incidence of wound infection is less than 5%. Except a very few conditions, non surgical antibiotic prophylaxis is not routinely indicated. Although awareness of the consequences of antibiotic misuse is increasing, overprescribing remains widespread. Overuse of antibiotics and poor compliance with infection control measures have been identified as the two major reasons for increasing antimicrobial resistance. [4] Studies on antibiotic prescription practices in ICUs have been done in some countries, [1,5] but information regarding studies done in Indian ICU setting is extremely limited. Antibiotic recommendations based on studies performed at a few selected centers may not be applicable and may not be generalized to all ICU settings. Singh N et al has suggested that research in individual ICU is essential in guiding antibiotic prescription practices. [6] As antibiotic policy for ICU in our Hospital was in developmental phase and we needed to know the potential areas of concern, a cross sectional study was done, to study the extent and pattern of use of antibiotics for prophylaxis in medical and surgical intensive care units.
MATERIAL AND METHODS
The Hospital, in which this study was conducted, is a 550 bedded tertiary care hospital. There are two adult ICUs, medical and surgical ICU, each ICU is a 12 bedded unit. In surgical ICU (SICU) majority of patients admitted are because of road traffic accidents and surgical patients admitted after various surgical procedures. In medical ICU majority of patients admitted are because of respiratory, cardiac or multiorgan failure.
Inclusion and exclusion criteria: Patients admitted in SICU and MICU, of age above 18 years, irrespective of sex were included in the study from October 2007 to October 2009. Patients whose relatives were not willing to give consent and patients with age less than 18 years were excluded from the study.
Collection of data: Permission was taken from Institutional Human Research Ethics Committee before starting the study. A total of 200 patients were included randomly, 100 from each ICU. As patients admitted in ICU are critically ill, written informed consent was taken from the relatives of the patients. Case record files of the included patients were analyzed daily until their discharge from ICU or a maximum of 21 days. Treatment was considered prophylactic if there was no evidence of infection and the drug was used to prevent infection. Details of all antibiotics prescribed for prophylaxis were recorded in a predecided proforma, including group of drug, route of administration, dose and duration of treatment.
Statistical analysis: Data was analysed on Microsoft excel 2007. Mean and frequencies were calculated in the two groups. Chi square test was used to compare proportions and p value of < 0.05 was considered as significant
RESULTS
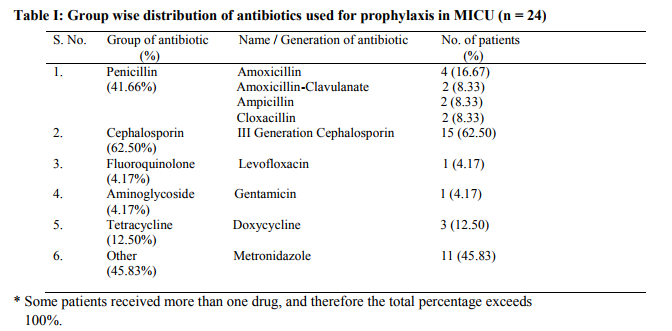
In MICU 65 (65%) patients were prescribed antibiotics either single or in combination while in SICU 99 (99%) patients were prescribed antibiotics (p value <0.0001). In MICU antibiotics consisted 15% of total drugs (excluding intravenous fluids) prescribed while in SICU 23.54% of total drugs prescribed (p value <0.0001). Out of 65 patients who received antibiotics in MICU, 24 (37%) received them for prophylaxis, while in SICU 72 (73%) out of 99 patients received antimicrobial prophylaxis (p value <0.0001). In MICU 4.6% received surgical prophylaxis and 33.8% received non surgical prophylaxis. In SICU 37% received surgical prophylaxis and 36% non surgical prophylaxis. Average duration of antimicrobial prophylaxis in MICU was 2.58 days and in SICU 5.24 days. Antimicrobial prophylaxis for more than 24 hours was given in 19 (79.14%) patients in MICU and in 48 (66.67%) patients in SICU (p value = 0.3690). In 13 (54.2%) patients in MICU and in 32 (44.4%) patients in SICU antimicrobial prophylaxis was used for more than 48 hours (p value = 0.5549). Third generation cephalosporins were the most commonly prescribed antibiotics for prophylaxis in both ICUs (62.5% and 83.33% in MICU and SICU respectively) followed by metronidazole (45.83%) in MICU and metronidazole (19.44%) and amikacin (19.44%) in SICU. Frequency of different groups of antibiotics used for prophylaxis in MICU and SICU is given in Table I and II respectively. Comparison of most commonly used antibiotic groups in both ICUs is given in Table III. Out of those patients who received antimicrobial prophylaxis, 15 (62.5%) patients in MICU while 31 (43%) patients in SICU received combination of antibiotics (p value = 0.156). Most common combination used in MICU was 3rd generation cephalosporin with metronidazole, while in SICU 3rd generation cephalosporin with aminoglycoside was the most common combination used for prophylaxis. Among patients who received antibiotics for prophylaxis, 6 (25%) patients in MICU and 22 (30.55%) patients in SICU, later received empirical therapy for suspected infection despite of antimicrobial prophylaxis (p value = 0.7954).
DISCUSSION
As patients in ICUs are critically ill and more susceptible to nosocomial infections, more frequent use of antibiotics in these units is expected. In a study done by Roder BL et al, total antibiotic consumption was approximately ten times greater in ICU wards than in other wards. [1] In our study also, antibiotics were frequently prescribed, 65% patients in MICU and 99% in SICU received antibiotics. Though use of antibiotics in MICU was in accordance with that reported by Roder BL et al and Bergmans DCJJ et al in their studies, [1,7] antibiotic use in SICU was far more prevalent, much higher than found in other studies. [1,7,8] Similarly prophylactic use of antibacterials was significantly less in MICU as compared to SICU; it was also less than reported by studies done in other countries, [1,5] where more than half of the patients received antimicrobial prophylaxis. The picture in SICU was different, where out of total patients who received antibiotics, 73% received antimicrobial prophylaxis, a figure much higher than found in above mentioned studies. The incidence of non surgical prophylaxis was almost similar in the two ICUs, as more surgical patients are admitted in SICU; surgical prophylaxis is mostly responsible for this difference. Many guidelines are available for surgical prophylaxis which recommend 1st generation cephalosporin as first choice and for not more than 24 hours. [3,9] Concerning non-surgical prophylaxis, excluding a few specific conditions like neutropenia, there is evidence for only two approaches that are oral decontamination and selective digestive decontamination (SDD). [10-12] Observations in our study were far away from these recommendations. Inappropriate antibiotics were prescribed for lengthy periods (mean duration 2.58 days in MICU and 3.14 days in SICU), and in too many patients. Instead of 1st generation cephalosporins which are recommended for surgical prophylaxis, 3rd generation cephalosporins were the most commonly used antibiotics in both ICUs. Antibiotic combinations were frequently used in both ICUs for prophylactic purpose. Providing broad spectrum coverage to patients might be a reason for high prevalence of use of antibiotic combinations. Oral decontamination and SDD were never used in this study for non surgical prophylaxis. Use of antibiotic prophylaxis in non-surgical patients except a few specified conditions is not recommended by any guidelines. This practice increases the chances of development of antibiotic resistance and induces a false sense of confidence in clinicians who consequently pay less attention to the possibility of occult infection. [5] This possibility correlates with the finding in our study that out of total patients who received antimicrobial prophylaxis, 6 (25%) patients in MICU and 22 (30.55%) patients in SICU later received empirical antibiotics for suspected infection despite of antimicrobial prophylaxis. Adherence to internationally accepted guidelines has been found low in other studies also. [5,13] There were some limitations in present study. Relatively small number of patients was studied in both intensive care units. As clinicians were not included in the present study frame, we can not conclude on the reasons responsible for nonadherence of antibiotic prescription practices to internationally accepted guidelines.
CONCLUSION
In the current scenario when antimicrobial resistance is growing in intensive care units and nosocomial infections are becoming more and more difficult to treat, appropriate and cautious use of antibiotics particularly in intensive care units becomes a necessity so that we can use these wonder drugs in future also. Present study has provided a baseline data of the prophylactic use of antibiotics in intensive care units of a tertiary care teaching hospital. Liberal use of antibiotics for surgical and non surgical prophylaxis, with broad spectrum antibiotics and antibiotic combinations, and for long durations, has emerged as areas of concern in present study. As characteristics of patient population, their risks and susceptibilities to various infections, as well as predominant pathogens and their antimicrobial resistance varies between different ICUs, such surveillance studies and research help in recognition of areas of special concern which can guide the formulation of antibiotic prescription policies at individual ICU level.
ACKNOWLEDGEMENT
We acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. We are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Roder BL, Nielsen SL, Magnussen P, Engquist A, Frimodt-Moller N. Antibiotic usage in an intensive care unit in a danish university hospital. J Antimicrob Chemother 1993;32:633-42.
2. Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, 1999. Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol 1999;20(4):250-78.
3. Chambers HF. General principles of antimicrobial therapy. In: Brunton LL, editor. Goodman and gilman‘s the pharmacological basis of therapeutics. 11th ed. New York: McGraw-Hill; 2006. p. 1095- 110.
4. Goldmann DA, Weinstein RA, Wenzel RP et al. Strategies to prevent and control the emergence and spread of antimicrobialresistant microorganisms in hospitals. a challenge to hospital leadership. JAMA 1996 Jan 17;275(3):234–40.
5. Malacarne P, Carlotta R, Bertolini G. Antibiotic usage in intensive care units: a pharmaco-epidemiological multicentre study. J Antimicrob Chemother 2004;54(1):221-4.
6. Singh N, Yu VL. Rational empiric antibiotic prescription in the ICU – clinical research is mandatory. Chest 2000;117(5):1496-9.
7. Bergmans DCJJ, Bontena MJM, Gaillardc CA et al. Indications for antibiotic use in ICU patients: a one-year prospective surveillance. J Antimicrob Chemother 1997;39:527-35.
8. Hartmann B, Junger A, Brammen D et al. Review of antibiotic drug use in a surgical ICU: management with a patient data management system for additional outcome analysis in patients staying more than 24 hours. Clin Ther 2004 June;26(6):915-24.
9. Lampiris HW, Maddix DS. Clinical use of antimicrobial agents. In: Katzung BG, editor. Basic and clinical pharmacology. 11th ed. Boston Burr Ridge (IL): The McGraw-Hill Companies; 2009. p. 827-41.
10. Marino PL. The ICU book. 3rd ed. Philadelphia (PA), USA: Lippincott Williams and Wilkins; 2007. p. 63-80.
11. Bergmans DCJJ, Bonten MJM, Gaillard CA et al. Prevention of Ventilator-associated Pneumonia by Oral Decontamination. A Prospective, Randomized, Double-blind, Placebo-controlled Study. Am J Respir Crit Care Med 2001 Aug;164(3):382-8.
12. Ulrich C, Harinck-de Weerd JE, Bakker NC, Jacz K, Doornbos L, de Ridder VA. Selective decontamination of the digestive tract with norfloxacin in the prevention of ICU-acquired infections: a prospective randomized study. Intensive Care Med 1989;15(7):424-31.
13. van Kasteren MEE, Kullberg BJ, de Boer AS, Mintjes-de Groot J, Gyssens IC. Adherence to local hospital guidelines for surgical antimicrobial prophylaxis: a multicentre audit in Dutch hospitals. J Antimicrob Chemother 2003;51:1389-96.

|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





