IJCRR - 4(16), August, 2012
Pages: 35-38
Date of Publication: 28-Aug-2012
Print Article
Download XML Download PDF
COMPLETE UNILATERAL DISCOID LATERAL MENISCUS IN AN ADULT CADAVER: A CASE REPORT
Author: C Ashwini, CM Nanjaiah, GS Saraswathi
Category: Healthcare
Abstract:The menisci and their attachments into bone represent a functional unit. The menisci are able to distribute loads and therefore reduce the stress on the tibia, a function which is regarded as essential for cartilage protection and prevention of osteoarthritis. Lubrication, proprioception and joint stabilization, load transmission are the major functions of the knee meniscus. Lateral meniscus tends to show more developmental variations. Among many types of meniscal anomalies reported, discoid meniscus is the most common entity. The etiology of discoid meniscus has only been partially explained. Here we report a case of unilateral discoid lateral meniscus which was observed in an adult male cadaver.
Keywords: Lateral Meniscus, Discoid, adult, knee joint.
Full Text:
INTRODUCTION
The menisci and their attachments into bone represent a functional unit. The menisci are able to distribute loads and therefore reduce the stress on the tibia, a function which is regarded as essential for cartilage protection and prevention of osteoarthritis.1 The traumatic lesions of the medial meniscus is more common than the malformation and degeneration, where as malformation is more common in lateral meniscus. Congenital abnormalities of menisci like complete absence of menisci, change in the shape of the menisci like C, U, V, and Discoid have been observed. Among many types of meniscal anomalies reported, discoid meniscus is the most common entity. Incidences of tears are more common in discoid menisci and absence of menisci leads to degenerative changes within the knee. The snapping knee syndrome, which appears more often in Children and Adolescents, is usually related with the type of the meniscus or to the presence of a tear of the meniscus.2, 3, 4 Here we report a case of unilateral discoid lateral meniscus which was observed in an adult cadaver.
MATERIAL AND METHODS
During routine dissection for I MBBS students we observed a Discoid lateral meniscus in an adult cadaver in a Department of Anatomy, JSS medical college, Mysore, India
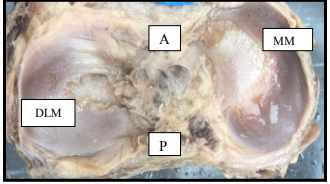
Figure 1: Photograph showing the complete lateral discoid meniscus of left knee joint. (DLM- Discoid lateral meniscus, MM- Medial meniscus, A- Anterior, P- Posterior) The complete type of Lateral discoid meniscus was found on the left side knee of the cadaver. It was disc shaped (fig 1) and occupying 90% of the tibial plateau. The meniscus was wider than usual and measuring 0.8cm, 1.3cm, 1.0cm in anterior one third, middle third and posterior third respectively. Measurements were taken by using a sliding caliper. Lateral meniscus on right side was normal. Medial menisci on both the sides were normal in shape.
DISCUSSION
The anatomical abnormalities and variations of the intraarticular structures of the knee joint have recently become significant because of new techniques available in diagnostic and surgical fields such as arthroscopy, computed tomography, magnetic resonance imaging and knee replacement surgery. The differential diagnosis of the lateral meniscal anomalies include discoid meniscus, ring shaped meniscus, double layered meniscus, hypoplastic meniscus, accessory meniscus, partially deficient meniscus and abnormal band of meniscus. Also the investigation of these variants is important in order to define the morphological features for clinical diagnosis and surgical interventions.2 Meniscal hyperplasias, or discoid menisci, have been the focus of many studies because they are frequently the source of symptoms. Corresponding to the condyles of the femur and tibial plateau, the normal morphology of the lateral and medial menisci differs from each other.5 The most commonly used classification system for discoid lateral menisci, by Watanabe, is based upon their shape and tibial attachments. This classification was developed from arthroscopic observations, divides discoid lateral menisci into three types, complete, incomplete, and Wrisberg ligament. If the meniscus occupies more than 80% of tibial plateau it is considered as complete type and less than 80% which is wider than usual is called as incomplete type. Type III DLM, the so-called ‘Wrisberg ligament type’, is more normal in morphology except for a thick posterior horn and they lack posterior capsular attachments other than the posterior meniscofemoral ligament.6 Smillie was the first to proposed the theory about the cause of the discoid meniscus, according to him it results from failure in the resorption of the central area of the cartilage plate during development.7 A study which was done in Japan to verify the developmental etiology significantly larger in fetuses on 41 human fetuses knee joint (from 14 to 30 weeks of gestation) and 14 adults (from 56 to 91 years of age) comparatively. They have observed that the proportion of the area covered by the meniscus in the tibial plateau is than in adults, suggesting that the incomplete type possibly originates from fetal morphology of the meniscus. While the areas of the medial meniscus and tibial plateau increased more rapidly than those of the lateral meniscus and tibial plateau, the ratio of the meniscus area to the plateau in the lateral side was constitutively larger than in the medial side. With their results they have concluded that the covered area of the tibial plateau by the meniscus during the fetal period is larger in the lateral side than in the medial side, which may contribute to the higher incidence of discoid meniscus in the lateral side.8 Le Minor JM reported that no embryological study in the human fetus had ever shown this initial discoid stage, the LM having its adult crescent shape from its inception. He added that the DLM did not originate by the persistence of a normal embryonic structure but resulted directly from abnormal morphogenesis.9 There are racial differences in the incidence of discoid lateral meniscus. Robert H, Miller (2003) reports that the incidence of discoid lateral meniscus has ranged from 26% to even less than 1%.10 In fetal cadaver study, Kale A et al (2006) reported that 77% of the lateral menisci were discoid (n=22). The reported incidence of discoid menisci has ranged from 0.4 to 17%, with the vast majority occurring on the lateral side of the knee. Cadaver studies have reported the prevalence of lateral discoid menisci to be between 0 and 7%, whereas arthroscopic studies have demonstrated ranges from 0.4 to 16.6%. 2 Murlimanju et, al. in fetal cadaver study has reported the incidence of discoid lateral meniscus as 17.9% in South Indian population.3 Murlimanju et al studied 54 lateral menisci in adult cadavers of Indian population for morphological variants. In their study there was no discoid lateral menisci. 11 In contrast, from a study conducted by P.S. Rao and S.K.Rao in South India, based on 3,167 knee arthroscopies done between the years1993 and 2004, 177 (5.59%) discoid lateral menisci were encountered.12 Compared with the normal meniscus, the discoid lateral meniscus has a higher frequency of meniscal tears, more so the solitary tears are more common. In meniscal allograft transplantation, it has been stated that providing a meniscal allograft that matches the size and shape of the meniscus to the recipient’s knee is the responsibility of the tissue bank providing the graft.
CONCLUSION
This is a case report of the discoid lateral menisci in an adult cadaver. Discoid lateral meniscus is a rare anomaly which is clinically important because of its higher incidence of tear. There are differences among authors regarding its etiology though most of the authors believe that it must be of congenital origin. We believe that this report discusses etiological factors, embryology and clinical anatomy of the discoid lateral meniscus. This report will be helpful for Orthopedicians during diagnosis and treatment.
ACKNOWLEDGEMENT
Authors sincerely thank Dr N M Shamsundar Professor and Head, Dept of Anatomy, JSS Medical College, Mysore for his constant support. Authors also acknowledge the immense help received from the scholars who articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors/ publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed
References:
1. Messner K, Gao J. The menisci of the knee joint. Anatomical and functional characteristics and rationale for clinical treatment. J of Anat.1998; 193:161-178.
2. Kale A, Kopuz C, Edyzer M, Aydin M.E, Demyr M, Ynce Y. Anatomic Variations of the Shape of the menisci: a neonatal cadaver study. Knee Surg Sports Traumatol Arthrosc. 2006; 14: 975-81.
3. Murlimanju BV, Nair N, Ray B, Pai M, Amin S, Pai SR. Morphological variants of lateral meniscus of the knee: a cadaveric study in South Indian human fetuses, Anat Sci Int.2011 June; 86(2): 63-8.
4. Murlimanju BV, Nair N, Ray B, Pai M, Amin S, Pai SR, Morphometric analysis of the menisci of the knee joint in South Indian human fetuses. Int. J. Morphol. 2010; 28(4): 1167-71.
5. Fukazawa I, Hatta T, Uchio Y, Otani H. Development of menisci of the knee joint in human fetuses. Congenital anomalies. Mar 2009; 49 (1): 27-32.
6. Kocher MS, Klingele K, Rassman SO. Meniscal disorders: normal, discoid and cysts. Ortho clin North Am.2003; 34: 320- 340
7. Smillie IS. The congenital discoid meniscus. J Bone Joint Surg Am. 1948; 30B: 671–682.
8. Kato Y, Oshida M, Aizawa S, Saito A, Ryu J. Mod Rheumatol. 2004; 14: 154-9.
9. Le Minor JM, Comparative morphology of the lateral meniscus of the knee in primates, J Anat, 1990, 170:161–171
10. Miller RH III Knee Injuries, Campbell’s Operative Orthopaedics, 10th edn, Mosby (Elsevier), Philadelphia, 2003; Vol 3:2182- 99.
11. B.V. Murlimanju, et al. Morphological study of the menisci of the knee joint in adult cadavers of the South Indian population Marmara Medical Journal 2010;23(2); 270- 275
12. Rao SK, Rao PS. Clinical, radiologic and arthroscopic assessment and treatment of bilateral discoid lateral meniscus. Knee Surg Sports Traumatol Arthrosc 2007; 15: 597- 601.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





