IJCRR - 4(24), December, 2012
Pages: 68-73
Print Article
Download XML Download PDF
EFFECT OF ULTRASOUND THERAPY WITH END RANGE MOBILIZATION OVER CRYOTHERAPY WITH CAPSULAR STRETCHING ON PAIN IN FROZEN SHOULDER - A COMPARATIVE STUDY
Author: Shahbaz Nawaz Ansari, I. Lourdhuraj, Shikhsha Shah, Nikita Patel
Category: Healthcare
Abstract:Background: Effectiveness of any individualized therapeutic modality in reducing pain in frozen shoulder is questionable and the combination of therapies has contradictory results. Objectives: The purpose of this study was to check the effectiveness between the treatment modalities of Ultrasound therapy and End range mobilization over Cryotherapy and Stretching as a treatment program in alleviating pain of patients with frozen shoulder. Methods: Forty subjects diagnosed to have frozen shoulder were randomly assigned to two groups. Subjects in Group I received Ultrasound therapy and End range mobilization of shoulder while subjects in Group II got Cryotherapy and Stretching of shoulder. Both the groups were treated for 6 days a week for 4 weeks. Response to pain was considered as the outcome measure. Results: Statistical analysis was done considering p< 0.05 as statistically significant and the„t? value were estimated. It was found that ultrasound therapy when combined with end range mobilization had„t? value of 1.8342 in comparison to that of cryotherapy combined with stretching group. Conclusion: Ultrasound therapy with end range mobilization produced a better result than cryotherapy with stretching in reducing pain and therefore can be recommended in the treatment of frozen shoulder.
Keywords: Frozen shoulder, ultrasound therapy, end range mobilization, cryotherapy, stretching
Full Text:
INTRODUCTION
Frozen shoulder clinically referred to as adhesive capsulitis has been described as a condition of “unknown etiology characterized by gradually progressive, painful restriction of all joint motion with spontaneous restoration of partial or complete motion over months to years”7 . Its clinical course is divided into stages of freezing, lasting from onset to between 10 and 36 weeks, characterized by severe pain and a gradual diminution of articular volume, frozen stage lasting between 4 and 12 months when pain decreases gradually but without appreciable improvement in motion and thawing stage which is marked by gradual return of motion and may last between 12 months to few years 10 . Ultrasound therapy (UST), one of the modalities used to treat frozen shoulder elevates tissue temperature to depths of more than 5 cm causing increased collagen tissue extensibility, pain threshold, and enzymatic activity. It also changes nerve conduction velocity, contractile activity of the skeletal muscle12. Cryotherapy is another important modality which controls pain by directly and rapidly modifying the sensation of pain and controlling the pain transmission with the activity of cutaneous thermal reception 3.
Frozen shoulder, an inflammatory condition where the movements are inhibited as a result of pain requires periodic mobilization and stretching. Mobilization techniques applied close to the articular surface in ventral, dorsal and inferior directions of the gleno-humeral joint are frequently used by physical therapists as an intervention for limited joint range of motion11 . Passive stretching is a therapeutic maneuver designed to lengthen pathologically shortened soft tissue by using an external force, applied either manually or mechanically for about 30 seconds and thereby facilitate increase in range of motion1 . Shoulder Pain and Disability Index (SPADI) is used to assess pain and routine functional skills of shoulder. A ten-point reduction in the score accurately distinguishes between people whose shoulder problems improve and those whose conditions remain stable and a ten-point gain distinguishes between people whose shoulder problems are unchanging and those whose problems are worsening 17 . Visual Analog Scale (VAS) provides a simple means of measuring subjective experience of pain and has been established as a valid and reliable tool in a range of clinic and research applications. VAS is one of the most frequently used measurement scale of pain in healthcare research and practice8 . There are various studies supporting the individual effects of ultrasound therapy, mobilization, Cryotherapy and capsular stretching in patients with frozen shoulder. However, combination of modalities has been less explored. This study attempts to find out the combined effect of Ultrasound therapy (UST) and End range mobilization (ERM) over cryotherapy and capsular stretching in reduction of pain in patients with frozen shoulder.
MATERIALS AND METHODS
All the participants in the study signed an informed consent form and the variable was recorded prior and after 4 weeks of intervention. Forty patients of either gender aged between 30 to 60 years and diagnosed to have frozen shoulder and a SPADI rating between 5 -6 since 2 months were randomized to two groups of 20 using block randomization after an initial screening for inclusion and exclusion criteria. Participants in group I underwent UST along with ERM and those in group II were given cryotherapy with capsular stretching as treatment strategies. Pain levels were estimated using a Visual Analogue Scale pre and post treatment and SPADI score was considered for inclusion. Participants known to have uncontrolled diabetes mellitus, orthopedic abnormalities around the shoulder and neuromuscular disorders were excluded.
PROCEDURE
Participants of group I were given pulsed ultrasound in sitting with a pulse ratio of 1:4 and an intensity of 1.5 W/cm2 for 10 minutes followed by end range mobilization (ERM) in loose pack position of the joint with participant in supine lying for a period of 20 minutes was given. The direction of mobilization was altered by varying the degree of rotation. Maitland mobilization grade 3–4 was administered for 2 minutes interspersed with a rest period of 30 seconds for 10-15 repetitions once a day, 6 days a week for 4 weeks 16 . Participants of group II were given cryotherapy using ice packs in the anterior, superior and posterior aspect of the shoulder for a period of 10 minutes followed by Capsular stretching and general stretching exercises of the shoulder for 20 minutes. This was administered once a day, 6 days a week for 4 weeks.
DATA ANALYSIS
Pre - post comparison between groups was done using Independent „t? test and that within the groups was analyzed using paired „t? test. The acquired „t? parameters are reported. The mean difference of pain in both groups was compared and the pattern of variation was observed. P value <0.05 was considered statistically significant for this study
RESULTS
In this study, the authors found a significant difference between the two groups to infer the effectiveness of UST and ERM over Cryotherapy and stretching in the treatment of patients with frozen shoulder. Forty participants with a mean age of 53.7 years and diagnosed with frozen shoulder were enrolled for the study. Participants in group I (15 men and 5 women) had a mean age of 53.8 ± 3.9 and those in group II (15 men and 5 women) were of 53.6 ± 4.8 years. Data was analyzed for the homogeneity between groups amongst pain using an independent „t? test. Analysis at p <0.05 revealed a „t? value of 0.1266 for shoulder pain which are not statistically significant in comparison to that of the table value 1.697 showing no difference between the groups. Table 1 shows the pre-post analyses of pain within and between groups using a dependent„t? test and independent „t? test respectively. Analysis showed statistically significant difference in the pre-post values in both groups and the difference within groups with p <0.05 was found to be more in UST + ERM group.
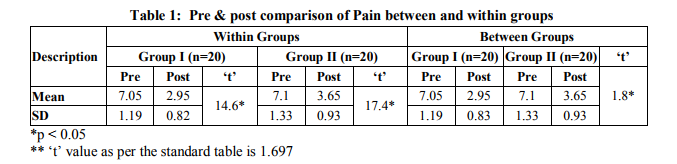
Pre-post analysis within group for pain reduction showed„t? values of 14.6408 and 17.3936 for group I and II respectively which are significantly higher than the table value of 1.729. Between group analysis using independent „t? test at p<0.05 showed significant difference between groups with the calculated „t? value of 1.8342 being more than the table „t? value of 1.697. However, the mean improvement in pain of shoulder between groups I and II are 4.1 and 3.45 respectively indicating the superior improvement in group I to that of group II.
DISCUSSION
This study done to investigate the effectiveness of Ultrasound therapy (UST) combined with End range mobilization (ERM) over Cryotherapy and capsule stretching showed an improvement in the pain status in patients with frozen shoulder. Literature states that frozen shoulder affects the joint which reduces the mobility as well as flexibility of the individual and the symptoms develop over 6 months, may last 2 years, and then gradually disappear (“self-limiting character”) 4, 5,14 . Sometimes, there may be long lasting pain and restricted motion12. Reeves10 described the natural history of frozen shoulder and found a mean duration of the disease of 30 months (range 12–42). Since in our patients? symptoms were present for at least 2 months, there is an indication that the changes seen after 2 months of treatment with ERM techniques could be attributed to the mobilization techniques rather than to the natural history of frozen shoulder. Vermeulen HM et al16 also opined that end range mobilization (Maitland “Grade 3-4”) plays a major role to get optimum movement of shoulder in conditions associated with frozen shoulder. The intention of giving ERM techniques in our patients was to stretch contracted peri articular structures as the authors believe that the exact time span for developing capsular contracture with adhesions is not known. End-range mobilization techniques can only be performed without causing too much pain if the inflammatory (first) phase has disappeared. The techniques authors used were mostly performed at the end of the ROM with a moderate, sometimes painful, intensity. In comparison to the observations made by other authors, 2,6,9,14,15 we saw no adverse effects on the recovery of patients with frozen shoulder treated with such mobilization technique. However the data should be interpreted with caution as there was no control group or measurements of the opposite shoulder for comparison. Robertson VJ et. al13 reported the usage of ultrasound therapy (UST) clinically in rehabilitation of patients with frozen shoulder. According to him, active therapeutic ultrasound is used for treating people with pain and musculoskeletal injuries to promote soft tissue healing. Both thermal and non-thermal effects of UST are proven beneficial in reducing inflammation and improve tissue extensibility, pain threshold, and enzymatic activity. The increased pliability of the tissue along with the reduction of inflammation as a part of thermal effects of UST paves way for aggressive mobilization of shoulder with low perception of pain. The non-thermal effects of UST have shown to reduce the recurrence of the symptoms also reducing the in-house rehabilitation duration. However, in the review by Robertson VJ et al 13, the author found that there is no substantial evidence for the therapeutic usage of UST in frozen shoulder. Hence authors of this study explored the combined effects of UST with ERM to enhance rehabilitation outcomes and derived the current conclusion. Research regarding connective tissue stretch duration and intensity has shown that high intensity, short duration stretching aids the elastic response, while low intensity, prolonged duration stretching aids the plastic response. There has been a direct correlation found between the resulting proportion of plastic, permanent elongation and the duration of a stretch and also the degree of either trauma or weakening of the stretched tissues and the intensity of a stretch. With these into consideration, authors opted to treat group II with capsular stretching along with cryotherapy. Cryotherapy, as had been well proven to be a modality in controlling pain by directly and rapidly modifying the perception and controlling the transmission to the higher centers can be used to treat painful shoulder syndromes like frozen shoulder.
The beneficial effect of ice therapy on reducing the inflammatory response adds on value to this modality as it primarily works by activating cutaneous thermal reception3 . The combination of therapies gave positive results in comparison to the individualized therapy which the authors attribute to the summative contribution of the physiological effects of each therapy in treating frozen shoulder. Authors feel that the duration of rehabilitation can be brought down by incorporating the combination therapies especially in a multifaceted pathology like frozen shoulder. Authors in this study found that both Ultrasound with end range mobilization and Cryotherapy with Stretching were effective in Group I and II. Though the results showed statistically significant improvement in pain parameter pre and post therapy in both the groups, the extent of improvement was noted better in Group I (UST + ERM) compared to Group II (Cryotherapy + Capsular stretching). Hence, they suggest that both combinations could be satisfactorily used to combat shoulder pain based on the availability of resources in the rehabilitation facility but the combination of UST and ERM stands the suggested treatment. The reduction in the extensibility parameters of the soft tissues around the joint and altered perception of the pain due to cryotherapy should have atleast contributed to the false improvement in the pain status. However, the findings disagree with the assumption and the improvement of pain was found better in group I where the subjects were treated with UST + ERM. This could be attributed to ERM after optimal warming and micro streaming effects of UST.
CONCLUSION
Study concludes that the subjects treated with Ultrasound therapy (UST) along with End range mobilization (ERM) showed better improvement in shoulder pain compared to those who received cryotherapy and stretching. This study was limited in its scope due to small sample size, lack of control group, shorter duration of treatment which the authors believe were important to comment on the prognosis of the patient using the given management strategy. Future studies with longer treatment duration and Pain and disability measured using more objective outcomes are recommended. However, this is just authors? hypothesis and could be investigated in detail by doing future trials involving larger sample.
ACKNOWLEDGEMENTS
Prof. Jasobanta Sethi, Dr. A. T. S. Giri, Dr. P. B. Balamurugan, Principal, Chairman, HOD, Goutham College of Physiotherapy Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Available from http://www.physioroom.com/prevention/stre tching3.php downloaded on 23rd Feb, 2006.
2. Bulgen DY, Binder AI, Hazleman BL, Dutton J, Roberts S. Frozen shoulder: prospective clinical study with an evaluation of three treatment regimens. Ann Rheum Dis. 1984; 43:353–360.
3. Forster A, Palastanga N. Clayton?s Electrotherapy. Bailliere Tindall/W. B. Saunders. Eastbourne, 1999; 9th edition: pp: 199-208. ISBN 0-7020-1100-2
4. Grey RG. The natural history of “idiopathic” frozen shoulder. J Bone Joint Surg Br.1978; 60:564.
5. Kay NR. The clinical diagnosis and management of frozen shoulders. Practitioner.1981; 225:164 –172.
6. Lewit, K. (1977) Manuelle Medizin im Rahmen der medizinischen rehabilitation. 2. Auflage. Johann Ambrosius Barth Leipzig.
7. Lori B Siegal, Norman J Cohen, Eric P Gall. Adhesive capsulitis: A Sticky Issue; Am Fam Physician.1999; 59(7):1843-50.
8. McCormack HM, Horne DJ, Sheather S. Clinical applications of Visual Analogue Scales: A critical review; Psychol Med.1988; 18(4): 1007-19.
9. Mens JM, de Wolf AN. Wat is de meest adequate behandeling van een zogenaamde frozen shoulder? Respons.1991; 2(10):1–3.
10. Reeves B; The natural history of the frozen shoulder syndrome. Scand J Rheumatol. 1975; 4(4): 193-196.
11. Rizk TE, Christopher RP, Pinals RS, Higgins AC, Frix R. Adhesive capsulitis: a new approach to its management. Arch Phys Med Rehabil. 1983; Jan; 64 (1): 29–33.
12. Robert A Donatelli, Micheal J and Wooden. Orthopedic Physical Therapy; 3rd ed, Churchill Livingstone publication. 2009; 153-158.
13. Robertson VJ, Baker KG. A review of therapeutic ultrasound - effectiveness studies, Physical Therapy. 2001; 81(7): 1339-50.
14. Rowe CR, Leffert RD. Idiopathic chronic adhesive capsulitis (“frozen shoulder”). In: Rowe CR, ed. The Shoulder. New York, Churchill Livingstone Inc. 1988; 155–163.
15. van der Korst JK. Periarthritis scapulohumeralis beschouwd vanuit de reumatologie. Nederlands Tijdschrift vor Fysiotherapi. 1980; 9:260 –263.
16. Vermeulen HM, Obermann WR, Burger BJ, Gea J Kok, Piet M Rozing, and Cornelia HM van den Ende. End-range mobilization techniques in adhesive capsulitis of the shoulder joint: a multiple-subject case report; Phys Ther 2000; 80:1240-1213.
17. Williams JW Jr, Holleman DR Jr, Simel DL. Measuring shoulder function with Shoulder Pain and Disability Index; J Rheumatol. 1995: 22(4): 727-32.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





