IJCRR - 5(5), March, 2013
Pages: 154-161
Date of Publication: 22-Mar-2013
Print Article
Download XML Download PDF
RENAL ARTERY VARIATIONS: A CADAVERIC STUDY WITH CLINICAL RELEVANCE
Author: Vrinda Ankolekar, Ratnabali Sengupta
Category: Healthcare
Abstract:Objectives: To observe and report the variations of renal artery in human cadavers. To compare the previous studies with the present study to report the incidence of the important type of variation. Methods: The study was performed on 60 cadaveric kidneys. The posterior abdominal wall was dissected in 30 embalmed cadavers to study the paired kidneys based on the method given in Cunningham's manual of practical anatomy Vol II. Results: The following parameters were observed. The number of renal arteries supplying each kidney, single in 73.33%, double in 23.33%, triple in 3.33%. The level of origin of renal arteries (RA), Right RA higher origin in 63.33%, Left RA higher origin in 10%, both right and left RA origin at same level in 26.7%. Branching of RA, Hilar in 88.33%, Prehilar in 11.67%. The prevalence of accessory renal arteries (ARA) in the present study is 25%. The percentage of unilateral ARA in the present study is 11.67% and of bilateral ARA is 6.67%. The percentage of arteries entering superior pole of the kidney, superior polar arteries (SPA) was 6.67%, inferior polar arteries(IPA) 10%, and hilar arteries(HA) 11.67%.. Percentage of origin of ARA from aorta is 20%, from main renal artery is 8.33%. Percentage of origin of SPA, IPA and HA from aorta is 3.33%, 8.33%, 8.33% and from main renal arteries is 2.33%, 1.67%, 2.33% respectively. Conclusion: Anatomical knowledge of the vascular variations is essential for the clinician to perform procedures such as renal transplantation, renal vascular operations more safely and efficiently.
Keywords: renal artery, accessory renal artery, cadaver, variations, parameters
Full Text:
INTRODUCTION
Renal arteries are a pair of lateral branches from the abdominal aorta below the level of superior mesenteric artery at the upper lumbar level (L1- L3). The paired renal arteries take about 20% of the cardiac output to supply the organs that represent less than one hundredth of total body weight. A single renal artery to each kidney is present in approximately 70% of individuals. Near the renal hilum, each artery divides into an anterior and a posterior division and these divide into segmental arteries supplying the renal vascular segments. Accessory renal arteries are common (30% of individuals), and usually arise from the aorta above and below the main renal artery and follow it to the renal hilum. They are regarded as persistent embryonic lateral splanchnic arteries1 . The frequency of accessory renal arteries show variability from 9%-76%. It is generally between 28%-30% in anatomic and cadaver studies. Variations or anomalies of veins are far more frequent than those of arteries, but this is not true of the vascular pedicle of the kidney-anomalous renal arteries are more common than are anomalous renal veins2 . Renal angiography, balloon angioplasty and stent implantation are now common diagnostic and therapeutic endovascular techniques in the treatment of renal artery pathology. For the successful implantation of the renal stent, precise knowledge of orientation of the origin of renal arteries from aorta is necessary. Multiple renal arteries have been associated with a higher rate of vascular complications, including arterial thrombosis and renal artery stenosis3 . Variations in the renal artery have been the subject of repeated study, and a voluminous literature exists. The subject however is well worth of further study, not only from the morphological but also from surgical point of view. But most of the studies have been based on ultrasonography and angiography, and it has been that accessory renal arteries are detected with less frequently in angiographic studies4 . Thus many workers, mainly surgeons have studied about the variations of renal arteries. This study was undertaken to observe and report the variations of renal arteries in humans, to compare the previous studies with the present study to report the incidence of important type of variation by cadaver dissection method.
MATERIALS AND METHODS
The study was conducted on 30 cadavers(60 kidneys) of both sexes during routine abdominal dissection for medical undergraduates, over a period of 3 years. Dissection was carried out to explore the vascular supply of kidney, along the length of abdominal aorta below the origin of superior mesenteric artery till its terminal bifurcation as common iliac arteries. Accessory renal arteries(ARA) were located and studied in detail and the specimens were photographed.
RESULTS
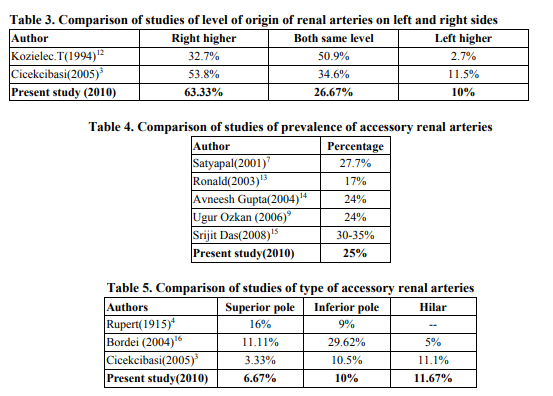
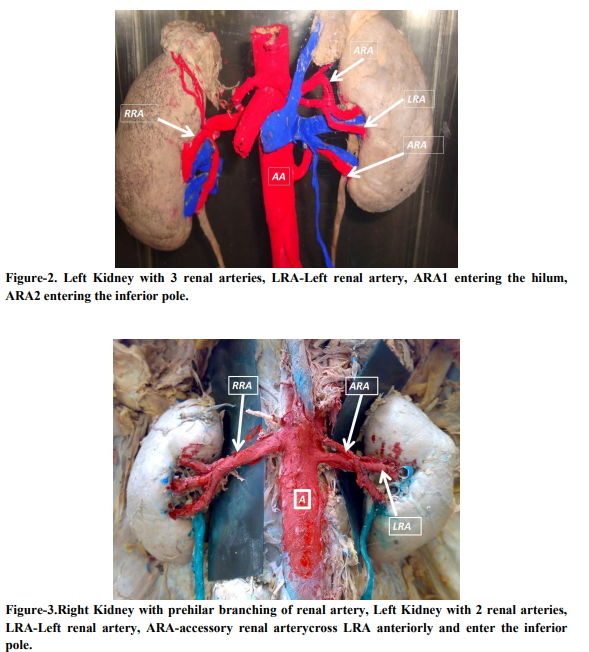
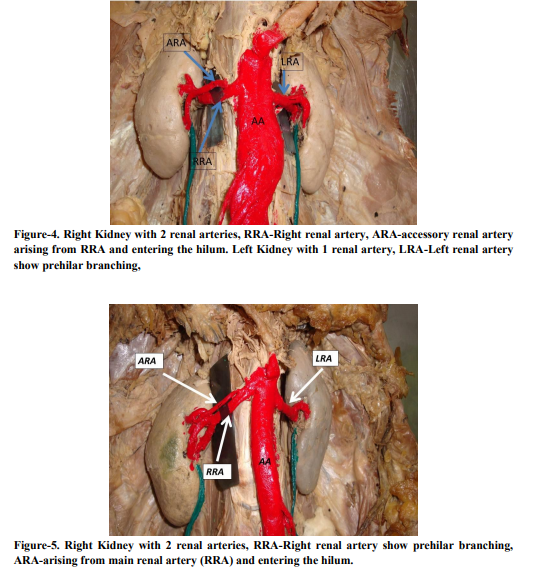
The following parameters were observed: A) Regarding the number of renal arteries entering the kidney: 2 arteries in 14 specimens (23.33%), 3 arteries in 2 specimens (3.33%). Fig 1 B) Regarding the level of origin of renal arteries (RA): The origin of right RA higher than the left RA in 19 specimens (63.33%), left RA origin higher than the right in 3 specimens (10%), both right and left renal artery origin at the same level in 8 specimens(26.67%). Fig 1&3 C) Regarding the branching of renal arteries: Hilar branching in 53 specimens (88.33%) Fig 1, Prehilar branching in 7 specimens (11.67%). Fig 3 right side D) Regarding the presence of accessory renal artery(ARA): ARA was found in 15 specimens (25%), 8 specimens on the right side. Fig 1, 4 & 5, 7 specimens on the left side. Fig 3 E) Regarding the prevalence of unilaterality or bilaterality of accessory renal arteries (ARA): Unilateral in 7 specimens (11.67%) Fig 2, 4 & 5, Bilateral in 4 specimens (6.67%). Fig 1 F) Regarding the type of accessory renal arteries (ARA): Superior polar arteries (SPA) are 5(6.67%) Fig 1 left side, Inferior polar arteries(IPA) are 6(10%) Fig 2 & 3 left side, Hilar arteries are 7(11.67%). Fig 4 G) Prevalence of type of accessory renal artery (ARA) on right side: superior polar arteries1(3.33%), inferior polar A-2(6.67%), hilar arteries-4(13.33%). Prevalence of type of accessory renal artery (ARA) on left side: superior polar A-3(10%), inferior polar A4(13.33%), hilar A-3(10%). H) Source of origin of ARA: Aorta-12 out of 17(20%) Fig 1, 2 & 3, Main RA-5 out of 17(8.33%) Fig 4 & 5, none from the common iliac artery or the bifurcation of aorta. I) Source of origin of different types of ARA: From Aorta-12, out of which 2 superior polar A, 5 inferior polar A, 5 hilar A. From Main Renal artery -5, out of which 2 Superior polar A, 1 Inferior polar A, 2 hilar artery.
DISSCUSSION
Knowledge of the variations of renal vascular anatomy has importance in exploration and treatment of renal trauma, renal transplantation, renovascular hypertension, renal artery embolisation, angioplasty or vascular reconstruction for congenital and acquired lesions3 . Abnormalities of renal arteries are perhaps more frequently noted than any other of the larger arterial trunks4 . The anomalies of accessory renal artery may be important from the clinical point of view in that they may cause a) hydronephrosis due to occlusion or compression of the ureter by an inferior polar artery, b) nephrotosis and malrotation of kidneys associated with an inferior polar artery, c) arterial hypertension because of constriction of renal artery and subsequent renal ischemia, d) the risk of infarction in a kidney during urologic or oncologic surgical interventions and renal transplantations. As the polar artery is a segmental artery, the erroneous ligation or division of it, is clearly hazardous resulting in necrosis of renal tissue5 . Knowledge of the wide variation in the arterial supply of the kidney is of utmost surgical importance, for it causes one to appreciate the hazard of too forcible traction on the vascular pedicle which may occasion rupture of an anomalous vessel and fatal hemorrhage6 . This statement pertains today especially since the definition of renal arterial anatomy impacts on renal transplant surgery, vascular operation for renal artery stenosis, reno-vascular hypertension, Takayasu’s disease, renal trauma and uroradiological procedures7 . .Renal arteries are usually single, one renal artery supplying each kidney. The frequency of extrarenal arteries shows variability from 9% to 76% and is generally between 28-30% in anatomic and cadaver studies8 . In our study, in 73.33% a single artery was found supplying the kidney, in 23.33% double renal artery, in 3.33% triple renal arteries. The results are similar to other studies (Table 1). The transplantation of kidney with the single artery is technically easier compared to the kidney with multiple arteries. On comparing the number of renal arteries on right and left side the present study is more comparable with that of the study conducted by Kozielec (Table 2). The extra renal arteries are detected much less frequently than angiography, and the arteries entering the renal parenchyma are frequently confused with adrenal or capsular arteries. So it is important to consider the results obtained by cadaver dissection method when compared to those obtained by angiographic method. Origin of right renal artery is usually higher than that of left. In our study, in 63.33% of specimens the right renal artery origin was at higher level, in 26.67% the origin of both right and left at the same level, in 10% the origin of left was at higher level (Table 3). Branching of renal arteries into anterior and posterior divisions more proximal than the renal hilar level is called early division9 . In present study, the division of renal artery was normal in 88.33% and early in 11.67%. This is comparable with the studies done by Kadir.S8 and Ugur Ozkan9 . Accessory renal arteries are common, and usually arise from aorta above or below the main renal artery and follow it to the renal hilum. They are regarded as persistent embryonic lateral splanchnic arteries1 (Table 4), compares the prevalence of accessory renal arteries in our study with other studies. The accessory renal arteries may be unilateral or bilateral. In our study the bilateral occurrence of accessory renal artery is 6.67%, and unilateral occurrence is 11.67% which is similar with the study by Dhar and Lal.(Unilateral-15%, Bilateral5%). The normal renal arteries enter the kidney through the hilum whereas the ARA may enter the kidney through the hilum other than its center or through the surfaces of the kidney. In our study the accessory renal artery were classified as superior polar artery, inferior polar artery, and hilar artery and the prevalence of these types was compared with those of other studies. The inferior polar arteries are of extremely important in several clinical and surgical conditions, such as hydronephrosis. The inferior polar artery may obstruct upper part of ureter or the ureteropelvic junction causing hydronephrosis1 . Accessory vessels to the inferior pole cross anterior to the ureter, and by obstructing the ureter may cause hydronephrosis1 . As the polar artery is segmental artery, the erroneous ligation or division of it, is clearly hazardous resulting in necrosis of renal tissue9 . Table 5 compares the studies noting the type of accessory renal arteries. The present study was compared with other studies regarding the prevalence of origin of types of accessory arteries. In our present study, out of 17 accessory renal arteries 12(20%) originated from aorta, whereas 5(8.33%) from the main renal artery. With the advent of laparoscopic renal surgeries and donor nephrectomies, it becomes mandatory for the surgeon to understand the abnormality or variations in the renal vasculature. Otherwise renal transplant may be jeopardized by the presence of accessory renal vessels. Therefore, considering the increase in incidence of the accessory and multiple renal arteries, the anatomical knowledge of such may be important for the academic, surgical as well as radiological procedures and the present study is a humble effort to highlight the same.
CONCLUSION
The results of the present study were discussed and it clearly indicates that the renal artery shows frequent variations. Most of the variations were in the origin, branching and presence of accessory renal artery. The accessory renal artery also shows wide variations in numbers, origin, course and branching. The knowledge of variations in renal arterial supply has wide clinical, surgical and academic implications. Familiarities about the possible variations are important to a surgeon dealing with kidney retrieval and transplantation, various endourological procedures and innumerable interventional techniques
ACKNOWLEDGEMENT
I sincerely express my gratitude to Dr. Ratnabali Sengupta for her valuable time, help, guidance, and valuable suggestions. I express my heartfelt gratitude to my colleagues Dr Suhani, Mrs Lydia, Dr Mamatha for their help and support. Authors acknowledge the great help received from the scholars whose articles cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Authors are grateful to IJCRR editorial board members and IJCRR team of reviewers who have helped to bring quality to this manuscript.
References:
1. Bannister LH, Berus MM, Collins P, Dyson M, Dusek JE, Ferguson MWJ. Grays Anatomy, 40th ed. Churchill Living Stone, Edinburgh; 2008. p. 1225-1233.
2. Hollinshead WH. Anatomy for Surgeons.Volume 2, New York: Harper and Row; 1971. p 533-546.
3. Cicekcibasi AE, Salbacak A, Seker M, Ziylan T, Buyukmumcu M, Tuncer I. An investigation of the origin, location, and variation of the renal arteries in human fetuses and their clinical relevance. Ann Anat; 2005. 187(4); p 421-427.
4. Rupert RR. Further study of irregular kidney vessels as found in 118 cadavers. SurgGynecObstet; 1915. 21: p 471 -480.
5. Necdet Kocabiyik, Bulent Yalgin, Cenk Kilig, Yalgin Kiric, Hasan Ozan. Accessory renal arteries and an anomalous testicular artery of high origin. Gulhane Tip Dergisi; 2005. 47: p 141-143.
6. Weinstein BB, Countiss EH, Derbes VJ. The renal vessels in 203 cadavers. UrolCutan Rev XLIV; 1940: p 137-139.
7. KS Satyapal, Haffejee AA, Singh B, Ramsaroop L, Roobs JV, Kalideen JM. Additional renal arteries: incidence and morphometry. J SurgRadiolAnat; 2001:23: p 33–38.
8. Kadir S. Kidneys. Atlas of normal and variant angiographic anatomy. Philadelphia: W.B.Saunders Company; 1991: p 387-429.
9. Ugur Ozkan, Oguzkurt Levent, Tercan Fahri, Kizilkiliç Osman, Koç Zafer, Koca Nihal. Renal artery origins and variations: angiographic evaluation of 855 consecutive patients. Diagnostic and interventional radiology (Ankara, Turkey); 2006:12(4): p 183-186.
10. Per Odman, Klaus Ranniger. The location of the renal arteries, an angiographic and post mortem study; Oct 1968:104: p 283-288.
11. K Khamanarong, P Prachaney, A Utararavivhien, T Tong Un, K Sripaoraya. Anatomy of renal arterial supply. Clinical anatomy; 2004:17(4): p 334-336.
12. Kozielec T. Variability in occurrence, course and division into branches of renal arteries in human fetuses. Ann Acad Med; 1994:40: p 109-116.
13. Ronald O Bude, Forauer AR, Caoili EM, Nghiem HV. Is it necessary to study accessory renal arteries when screening the renal arteries for renovascular hypertension?. J Radiology; 2003; 226: p 411–416.
14. Avneesh Gupta, Richard Tello. Accessory renal arteries are not related to hypertension risk; A review of MR angiography data. American Roentgen Ray Society; 2004:182: p 1521-1524.
15. Srijit Das. Anomalous renal arteries and clinical implications. BratislLekListy; 2008:109(4): p 182-184.
16. Bordei P, Sapte E, Iliescu D. Double renal arteries originating from the aorta. SurgRadiolAnat; 2004: 26(6): p 474-479.


|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





