IJCRR - 5(8), April, 2013
Pages: 47-52
Date of Publication: 25-Apr-2013
Print Article
Download XML Download PDF
SERUM URIC ACID AS A MARKER FOR MICROALBUMIN- URIA IN PREHYPERTENSION GROUP
Author: Anjaneya Prasad V., Vasu Babu N., Pradeep Babu K.V.
Category: Healthcare
Abstract:Background: Development of target organ damages like chronic kidney disease and coronary artery disease in hypertension is more common and more rapid. Identifying sub clinical target organ damage in prehypertensive phase is essential to prevent complications. Objective: Prehypertension is an elevation of systolic blood pressure of 120 - 139 mmHg and diastolic blood pressure of 80 \? 89mmHg. The purpose of this case \? control study was to corelate serum uric acid levels in Prehypertensive patients to the presence or absence of microalbuminuria. Method: This study was done at the Department of Internal Medicine, DR. PSIMS and RF foundation, Chinaoutpally, A.P.India between Jan 2011 to Dec 2012. 1000 patients (500 cases, 500 controls) above 18 years of age were included in the study. The microalbuminuric reference range was 30 \? 300mg/day. The reference values for serum Uric acid levels in males: 3.4 \? 7.0mg/dl and females were 2.4 \? 5.4mg/dl. Results: In our study, the microalbuminuria was present in 17.4% of prehypertensive cases and 3.4% of controls (p=0.0001), with mean value of microalbuminuria in cases was 30.91 + 16.54 and in controls was 7.191 + 6.039 (p = 0.0001). The mean serum uric acid levels in Prehypertensive group was 5.107 + 2.286 and in controls was 2.614 + 1.58 (p < 0.05), The mean serum uric acid levels in Prehypertensive group with microalbuminuria was 7.187 + 1.65 and in normoalbuminuria was 4.669 2 + 2.157 (p< 0.05). Conclusions: Serum uric acid levels were found to be significantly higher in Prehypertensive patients with microalbuminuria than without microalbuminuria.
Keywords: Prehypertension, Microalbuminuria, Serum uric acid
Full Text:
INTRODUCTION
The association between elevated serum uric acid level and cardiovascular disease risk was established by several large epidemiological studies.1 The causal role of uric acid in Cardiovascular risk was direct or indirect influence studied by different investigators.2 Elevated serum uric acid levels are associated with cardiovascular disease, particularly in hypertensive individuals due to endothelial dysfunction by reduced nitric oxide levels, decreasing neuronal nitric oxide synthase in the kidney, and activation of the renin-angiotensin system 3. Later studies, the development of renal microvascular changes, in which the thickened afferent arterioles and renal microvasculature hyalinosis , independently of hypertension and is likely to direct effects of high serum uric acid levels, which in turn stimulates and proliferation of vascular smooth muscle 4. The presence of direct or indirect effects of uric acid on microvasculature producing endothelial dysfunction, which in turn triggers hypertension cascade 5,6. By presence of this association of uric acid and hypertension, the risk of cardiovascular complications occurs rapid and severe. The diagnosis of hypertension in earlier phase i.e. Prehypertension, by JNC 7 definition: elevation of systolic blood pressure of 120 - 139 mmHg and diastolic blood pressure of 80 – 89mmHg 7, is useful to avoid subclinical cardiovascular risk and complications. Risk of progression to hypertension and risk of development of strokes are minimized by early detection of pro inflammatory markers and induction of early treatment schedules.
Microalbuminuria, by definition, excretion of albumin with urine in small amounts i.e. 30 – 300mg/day 8 influenced by wide range of confounding factors like increased body mass index, increased blood pressure (systolic, diastolic), blood glucose, C- reactive protein, altered lipid levels, hyperinsulinemia, smoking,Salt sensitivity and elderly individuals 9. Studies showed the significance microalbuminuria leads to pathogenesis of cardiovascular disease, by means of development of atherosclerotic vascular disease by systemic pathophysiological processes like activation of inflammatory mediators, Increased transcapillary escape rate of albumin and Vascular endothelial dysfunction 10.
Microalbuminuria is a well known marker of subclinical cardiovascular and renal disease as well as vascular endothelial dysfunction, in patients with diabetes, hypertension and general population. The effect of hyperuricemia on microalbuminuria in Prehypertensive phase can indirectly reflect its importance as a prognostic marker for long term complications of cardiovascular system even before the diagnosis of hypertension is made. The relationship between uric acid and microalbuminuria in Prehypertensive patients without other cardiovascular risk factors may help to clarify the role of uric acid in cardiovascular disease.
On this background, our study aims at comparing the occurrence of hyperuricemia in patients with Prehypertensive group with and without microalbuminuria, thus, reflecting presence or absence of any additive effect of hyperuricemia in Prehypertensive phase in causing major vascular complications.
MATERIAL AND METHODS
A prospective study was undertaken in the Department of General Medicine with the investigatory aid of Department of Biochemistry in Dr.PSIMSandRF, Chinoutpally, Gannavaram, Krishna (Dt.), Andhra Pradesh.
500 diagnosed Prehypertensive cases, who attended to our hospital and 500 age, sex matched controls, were included in our study group. All patients survive till the end of the study period of two years duration i.e., Jan 2011 to Dec 2012.
Diagnosis of Prehypertensive cases was done as per the JNC 7 guidelines.
Microalbuminuria in both cases and controls were estimated. Serum Uric acid and Lipid profile were also estimated in both cases and controls. The study was approved by the Ethics committee of our college. After fulfilling the inclusion and exclusion criteria, prior consent was obtained from the subjects.
Inclusion criteria
Patients with Systolic blood pressure: 120 – 139mmHg, Diastolic blood pressure : 80 – 89mmHg
Age 18 or older
Exclusion criteria
Patients with diabetes, heart failure, acute febrile illness, renal, hepatic, malignant disorders, chronic illnesses, asymptomatic infections and smokers.
Sample collection and analysis
Both heparinised and plain blood samples were collected from each case and control. For analysis of FBS, lipid profile - serum was used and for HBA1c – whole blood was used. Serum glucose estimation was done by Trindler’s Glucose Oxidase – Peroxidase (GOD – POD) method (commercial kit – ERBA – MANNHEIM), cholesterol estimation was done by Cholesterol Oxidase – Peroxidase (CHOD – POD) method (commercial kit – ERBA – MANNHEIM), Triglycerides estimation was done by Glycerol peroxidase (GPO) method (commercial kit – ERBA – MANNHEIM), HDL cholesterol estimation was done by apolipoprotein (APO) precipitation or Phospho Tungstic Acid (PTA) method (ERBA – MANNHEIM), and HBA1c estimation was done by Ion exchange resin method (commercial kit – Randox Rx series). All these estimations were performed by Randox Daytona Autoanalyzer. VLDL-c or LDL-c levels of all cases and controls were calculated by using Friedwald’s formula.
Estimation of serum uric acid was done by ERBA Chem 7 (Trans Asia) Semi Automatic analyzer and Autopak kits from Bayer Diagnostics India Ltd.
Urine samples from 24 – hour collected specimens were taken from each case and control and microalbumin estimation was done in those samples by Latex turbidimetry method (commercial kit-Euro diagnostic systems) on Randox Daytona Autoanalyzer.
RESULTS
The microalbuminuria was present in 17.4% of prehypertensive cases and 3.4% of controls (p=0.0001), which showed microalbuminuria is more frequent in prehypertensive cases than controls. Among in males, 68 (22.2%) in cases and 13(4.24%) in controls showed microalbuminuria that was statistically significant (p=0.0001). Among in females, 19 (9.79%) in cases and 4 (2.06%) in controls showed microalbuminuria that was statistically significant (p=0.0026).
The mean microalbuminuria in cases was 30.91 + 16.54 and in controls was 7.191 + 6.039 (p = 0.0001) which showed microalbuminuria is more frequent in Prehypertensive group, among in males mean microalbuminuria in cases was 32.55 + 11.96 and in controls was 7.459 + 6.382 (p = 0.0001), among in females mean microalbuminuria in cases was 28.31 + 7.77 and in controls was 6.769 + 5.445 (p < 0.05) were showed statistically significant mean microalbuminuria levels in males and females in cases than controls.
The mean serum uric acid levels in Prehypertensive group was 5.107 + 2.286 and in controls was 2.614 + 1.58 (p <0.05) which showed serum uric acid levels is more significant elevation in Prehypertensive cases, among in males mean serum uric acid levels in cases was 5.789 + 2.255 and in controls was 2.703 + 1.738 (p <0.05), among in females mean serum uric acid levels in cases was 4.03 + 1.89 and in controls was 2.47 + 1.28 (p<0.05) were showed statistically significant mean serum uric acid levels levels in males and females in cases than controls.
The mean serum uric acid levels in Prehypertensive group with microalbuminuria was 7.187 + 1.65 and in normoalbuminuria was 4.669 2 + 2.157 (p<0.05), which showed serum uric acid levels were statistically significant elevation in microalbuminuria with prehypertensive group.
The mean cholesterol in cases was 174.86 ± 29.9 and in controls was 167.3 ± 18.74 (p<0.05) which showed cholesterol is more significant elevation in Prehypertensive cases, The mean triglyceride level in cases was 152.2 ± 76.7and in 122.3 ± 47.6 controls was (p <0.05) which showed mean triglyceride level is more significant elevation in Prehypertensive cases, The mean LDL – cholesterol level in cases was 112.18 ± 25.3 and in controls was 96.64 ± 11.7 (p <0.05) which showed mean LDL – cholesterol level is more significant elevation in Prehypertensive cases, The mean HDL – cholesterol level in cases was 35.72 ± 7.48 and in controls was 40.32 ± 8.64 (p <0.05) which showed mean HDL – cholesterol level is more significant lowered in Prehypertensive cases.
The complications of Prehypertensive group were noticed in 3 – 7.6% patients than in controls (0%), among complications wise, ECG left ventricular hypertrophy changes were noticed in 7.6 % than controls (0%) (p=0.0001), and eye fundus changes were noticed in 3% than controls (0%) (p=0.0003) was statistically significant.
DISCUSSION
In this study, serum uric acid was associated with an increased risk of microalbuminuria in prehyertensive patients. Although many studies have previously shown the association between hyperuricemia and microalbuminuria in hypertensive patients13,14. This study has shown association in prehypertensive patients. Mild hyperuricemia induces endothelial dysfunction and activation of the renin angiotensin system (RAS), thus stimulating vascular smooth muscle cell (VSMC) proliferation 12.The mean age in prehypertensive group was 47.92 ± 9.36, and 81.8% prehypertensives were noticed more between the age group of 31 – 60 years.This study shows the mean serum uric acid was more in prehypertensive group(5.107) compared to normal subjects (2.073) ,when compared with Meena et al study,11 the results were similar that is more in prehypertensive group. Mean microalbuminurea levels were more in prehypertensives (30.91) compared to controls (7.19). Microalbuminurea was seen in 17.4% of prehypertensives and hyperuricemia was seen in 16.8% of the prehypertensive group.Males showed increase in mean serum uric acid levels and microalbumin levels compared to females in prehypertensive group. Serum total cholesterol, triglycerides and LDL were elevated in prehypertensive group compared to controls and HDL levels were decreased in prehypertensive group compared to controls.some complications like left ventricular hypertrophy and fundal changes were seen in prehypertensive group compared to controls.
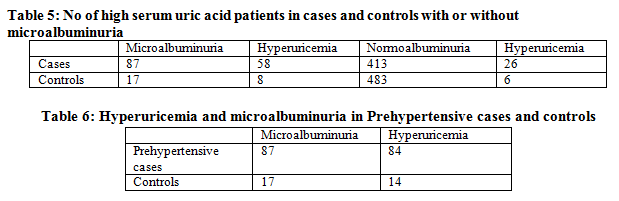
Among 87 patients with microalbuminuria 58 patients (66.6%) have hyperuricemia and only 26 patients(6.29%) showed hyperuricemia in 413 patiens with normoalbuminuria with a p value of 0.0001.Among 17 controls with microalbuminurea only 8 people(47%) have hyperuricemia and 6 controls (1.2%) showed hyperuricemia in 483 controls with normoalbuminurea with a p value of 0.0001.
When compared to study by Jung EL et al,1 this clearly shows that serum uric acid was elevated in prehypertesives as is microalbuminuria , and the hyperuricemia was noticed in microalbuminuruc prehypertensives .The possible mechanism presumed to be increased serum uric acid level combined with prehypertension might cause an endothelial dysfunction and result in glomerular hypertension, which would induce microalbuminuria and hyperfiltration 11.
In this study, we observed that elevated serum uric acid level was strongly associated with microalbuminuria among prehypertensive subjects without a history of cardiovascular disease or renal dysfunction.
CONCLUSIONS
Microalbuminuria levels were found to be significantly higher in prehypertensive patients by 17.4%. 81.8% of prehypertensive patients belongs to 31 – 60 years age group. Male to female ratio were found to be 1.57: 1.In prehypertensive patients with microalbuminuria group had elevated serum uric acid level in 66.6%. Prehypertesives with high mean microalbuminuria and high mean serum uric acid levels with significant elevated lipid levels had developed significant complications. Larger studies are required to clarify the significance of development of complications and to consider the microalbuminuria and serum uric acid are regular and routine screening markers to identify sub clinical target organ damage.
Declaration on conflict of interest
I declare that no conflicts are involved in this study.
ACKNOWLEDGEMENT
Authors acknowledge the great help received from the scholars whose articles cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Authors are grateful to IJCRR editorial board members and IJCRR team of reviewers who have helped to bring quality to this manuscript.

References:
- Lee JE, Kim YG, Choi YH et al. Serum uric acid is associated with microalbuminuria in prehypertension. Hypertension 2006; 47: 962–967.
- Johnson RJ, Kivlighn SD, Kim YG, Suga S, Fogo AB. Reappraisal of the pathogenesis and consequences of hyperuricemia in hypertension, cardiovascular disease, and renal disease. Am J Kidney Dis. 1999;33:225–234
- Mazzali M, Hughes J, Kim YG, et al. Elevated uric acid increases blood pressure in the Rat by a novel crystal-independent mechanism. Hypertension 2001; 38:1101–1106.
- Mazzali M, Kanellis J, Han L, et al. Hyperuricemia induces a primary renal arteriolopathy in rats by a blood pressure-independent mechanism. Am J Physiol Renal Physiol 2002; 282:F991–F997.
- Erdogan D, Gullu H, Caliskan M, et al. Relationship of serum uric acid to measures of endothelial function and atherosclerosis in healthy adults. Int J Clin Pract 2005; 59:1276–1282.
- Zoccali C, Maio R, Mallamaci F, Sesti G, Perticone F. Uric acid and endothelial dysfunction in essential hypertension. J Am Soc Nephrol 2006; 17:1466–1471.
- The Seventh Report of the Joint National Committee on hypertension
- Bennett PH, Haffner S, Kasiske BL et al. Screening and management of microalbuminuria in patients with diabetes mellitus: recommen- dations to the Scientic Advisory Board of the National Kidney Foun- dation from an ad hoc committee of the Council on Diabetes Mellitus of the National Kidney Foundation. Am J Kidney Dis 1995; 25: 107-12.
- Syamala S, Li J, Shankar A. Association between serum uric acid and prehypertension among US adults. J Hypertens. 2007;25(8):1583-
- Yong Loo Lin School of Medicine, National University of Singapore, Singapore Microalbuminuria: marker of vascular dysfunction, risk factor for cardiovascular disease Vascular Medicine 2002; 7: 35±43
- Meena CL,Harsha R,Meena VK,Anju B, Rajani N,Meena LP et al, Association of serum uric acid and microalbuminuria in prehypertension:Across sectional study. National journal of physiology, pharmacy and pharmacology 201; 3(1):87-91.
- Francesca Viazzi, Giovanna Leoncini, Elena Ratto, Valeria Falqui,Angelica Parodi, Novella Conti, Lorenzo E. Derchi, Cinzia Tomolillo,Giacomo Deferrari, and Roberto Pontremoli. Mild Hyperuricemia and Subclinical Renal Damage in Untreated Primary Hypertension. AJH 2007; 20:1276–1282.
- Viazzi F, Parodi D, Leoncini G, Parodi A, Falqui V, Ratto E, Vettoretti S, Bezante GP, Del Sette M, Deferrari G, Pontremoli R. Serum uric acid and target organ damage in primary hypertension. Hypertension. 2005;45:991–996.
- Mattei P, Arzilli F, Giovannetti R, Penno G, Arrighi P, Taddei S, Salvetti A. Microalbuminuria and renal haemodynamics in essential hypertension. Eur J Clin Invest. 1997;27:755–760.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





