IJCRR - 5(3), February, 2013
Pages: 54-61
Date of Publication: 18-Feb-2013
Print Article
Download XML Download PDF
ENERGY BALANCE, PSYCHOSOCIAL PROBLEMS AND BIOCHEMICAL PROFILE OF OBESE CHILDREN
Author: Kalpana C.A., Lakshmi U.K.
Category: Healthcare
Abstract:Childhood obesity is reaching epidemic proportions in both developed and developing countries. Reduced physical activity and increased energy intake both have major contribution to the establishment of childhood obesity. Psychological and social problems, increased plasma insulin, elevated blood lipid, lipoproteins and blood pressure are the various factors known to be associated with childhood obesity. Hence, the study was conducted to determine the energy balance, psychosocial problems and biochemical profile of selected obese children. Time utilization pattern of obese boys and girls (n=64) was studied to assess their physical activity and energy expenditure levels. The energy balance was calculated by finding the difference in the energy intake and energy expenditure of the children. Psychosocial and behavioural adjustment problems faced by obese children at school and home were studied for both the boys and girls. Biochemical parameters namely blood glucose, haemoglobin and lipid profile which included total cholesterol, serum triglycerides, HDL, LDL and VLDL cholesterol were determined using standard procedures. Both boys and girls exhibited a positive energy balance which was higher in obese boys than in obese girls. The mean total cholesterol level of obese boys (158.3 mg/dl) was within the normal range but in the case of obese girls the level (178.7 mg/dl) was found to be slightly higher than the normal. Overweight and obese children are likely to develop lifestyle diseases like diabetes mellitus and cardiovascular diseases at a younger age which are largely preventable. Strategies aimed at reducing caloric intake and increasing caloric expenditure through regular exercise are necessary to meet the challenges.
Keywords: Childhood obesity, energy balance, psychosocial problems, biochemical profile
Full Text:
INTRODUCTION
Obesity is reaching epidemic proportions in both developed and developing countries and is affecting not only adults but also children and adolescents [1].Once considered a problem of affluence, obesity is fast growing in many developing countries also. As a result of rapid socioeconomic advancements in recent decades, the population is undergoing significant changes in lifestyle, dietary and meal patterns, such as increased consumption of fats and oils, decreased intake of complex carbohydrates, eating out and skipping meals. Both physical activity and energy intake have a major contribution to the establishment of childhood obesity [2]. Sleep duration may be related to a child’s exposure to obesity related factors in the environment [3]. Physical health risk of obesity may not manifest themselves for years but the psychological and social problems are experienced every day. Obese children often suffer from teasing by their peers. Some are harassed or discriminated by their own family. [4]. Obesity is a key factor for many chronic and non communicable diseases. Increased plasma insulin levels, elevated blood lipid and lipoprotein levels, and elevated blood pressure are the various factors known to be associated with childhood obesity leading to adult morbidity and mortality. [5]. Childhood obesity prevention involves maintaining energy balance at a healthy weight, while protecting overall health, growth and development and nutritional status. Interventions that combine a dietary component, physical exercise and/or behavioural therapy are effective in treating childhood obesity. Hence, the study was conducted to determine the energy balance, psychosocial problems and biochemical profile of selected obese children.
MATERIALS AND METHODS
Childhood obesity is associated with a number of problems and co-morbidities; hence the following parameters were studied on 32 obese boys and 32 obese girls.
1. Assessment of Physical Activity Pattern Time utilization pattern of both obese boys and girls (n=64) was studied to assess their physical activity and energy expenditure levels. An equal number of normal boys and girls (n=64) were also assessed for their time utilization pattern for comparison with the obese children. For studying the time utilization pattern, each child was asked to prepare an activity time log for a week stating the time spent on each activity from the time one gets up in the morning to the time one goes to bed. The activities were then classified into sedentary, moderate and heavy based on the type of activity. The time spent for each type of activity was calculated for the whole day along with the time spent for sleep for determining the difference in activity pattern and sleep hours of obese children.
2. Determination of Energy Balance Energy balance is the state in which an individual’s energy expenditure equals his or her metabolizable energy intake. Negative energy balance occurs when expenditure is greater than intake and positive energy balance occurs when intake is greater than expenditure. Hence, an in depth study on energy balance was carried out on the 64 obese children. Basal Metabolic Rate (BMR) and physical activity are the two major factors which determine the energy expenditure of an individual. The energy expenditure of the obese children was assessed using the time utilization pattern. The average workload per day was computed with the number of hours spent for each activity in school and at home along with hours spent for sleep. Energy expenditure for sedentary, moderate, heavy activities and sleep was determined using the formula [6]
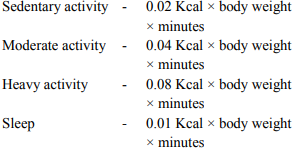
The basal energy requirement is regularly estimated as the energy need per kg of body weight which is assumed as one calorie for every hour per kilogram of body weight. Thus the basal energy expenditure for 24 hours for children is calculated as 1 X 24 X body weight. Energy that is saved during sleep is calculated as 0.1 X body weight X hours of sleep. This is reduced from the total basal energy expenditure for 24 hours to get the basal energy expenditure of the individual. Total Energy Expenditure (TEE) was calculated from the Basal Metabolic Rate (BMR) and the type of physical activities of the children. The actual food intake was determined from 24 hour recall method. From the average daily food intake, the energy intake was computed using the nutritive value of Indian foods and compared with the recommended dietary allowances [7]. The energy balance was thus calculated by finding the difference in the energy intake and energy expenditure of the children.
3. Psychosocial and Behavioural Adjustment Problems
Obesity is a stigmatized condition. Obese children are exposed to the consequences of public disapproval for their fatness. This stigma is seen in schools, homes and in the society. Hence, the psychosocial and behavioural adjustment problems faced by obese children at school and home were studied for both the boys and girls. Based on the scale developed by Parikh and Das [8], a Psychosocial and Behavioural Adjustment Scale (PSBA Scale) was constructed by the investigator after identifying 60 relevant statements through review of literature and in consultation with psychology experts and categorizing into six groups with equal number of positive and negative statements. Self perception of physical attributes, behaviour in the family, emotional and behavioural problems, social and academic problems and problems with values and adjustment were the aspects included in the development of this scale. The children were asked to respond to each statement in terms of their own agreement and disagreement on a five point continuum. The scores given for positive statements were as follows:
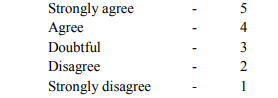
The order was reversed for the negative statements. The total score was the summation of numerical weight assigned to each response. This 5 point scale was given scores of 1,2,3,4 and 5 with 5 being the maximum score indicating least problems and 1 being the lowest score indicating most problems.
4. Biochemical profile
Biochemical parameters namely blood glucose, haemoglobin and lipid profile which included total cholesterol, serum triglycerides, HDL, LDL and VLDL cholesterol were determined in the laboratory for the selected children (n=64) using the following standardized methods.
a. Blood Haemoglobin
An accurate volume of blood (0.02ml) was drawn from a finger prick using a haemoglobin pipette and delivered on to a (1x1 cm) strip of Whatman No.1 filter paper. The filter paper with the blood sample was dropped into Drabkin’s solution in a test tube and allowed to stand for 30 minutes. The solution was then centrifuged and the supernatant was read in a photo electric colorimeter. The mean haemoglobin levels were then compared with reference values.
b. Blood Glucose
A finger prick was done for the selected overweight and obese children to collect their blood sample and blood glucose was estimated using a Glucometer.
c. Blood lipid profile
With the help of a laboratory technician, 5ml of blood was drawn from the vein of obese children and blood lipid profile comprising of Total cholesterol, Triglycerides, Low density Lipoprotein, High density Lipoprotein and Very Low Density Lipoprotein was estimated using standard procedures.
d. Blood Pressure
Obesity and overweight may predispose children to increased blood pressure. Elevated blood pressure in children is an early risk factor for cardiovascular disease and is positively associated with BMI [10]. Hence, blood pressure was measured for the selected obese children (n=64) with the help of an experienced medical officer.
RESULTS AND DISCUSSION
1. Mean hours spent on physical activities by Obese and Normal children
The mean hours spent in various physical activities during the day by obese boys and girls in comparison with normal children are presented in Table I.
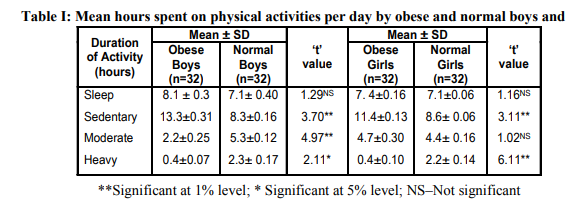
The duration of sleep hours per day for obese boys was 8.1 and for normal boys were 7.1 with no significant difference. The hours spent per day on sedentary activities among obese boys was found to be higher by 13.3 hours compared to only 8.3 hours spent by normal boys which was found to be statistically significant (p<0.01). The time spent per day in moderate activity by the obese boys was only 2.2 hours than the normal boys who spent 5.3 hours and the findings were found to be significant (p<0.01). A lesser and negligible time of 0.4 hours was spent by the obese boys per day on heavy activities when compared with normal boys who spent 2.3 hours and the difference was statistically significant (p<0.05). Sleep hours of both obese (7.4) and normal girls (7.1) showed no statistically significant difference. Obese girls spent significantly more time of 11.4 hours on sedentary activities when compared to the normal girls who spent only 8.6 hours and found to be significant (p<0.01). The time spent on moderate activities by obese girls was 4.7 hours and by normal girls was 4.4 hours daily and the difference was not significant. The duration of time spent on heavy activities by obese girls was comparatively very less (0.4 hours) than the normal girls who spent 2.2 hours with a significant difference (p<0.01). Obese children spent less time on house hold work and active transport and also performed less moderate/vigorous activities, but they spent longer times on low intensity activities, including leisure time reading, computer use, video games, study and inactive transport [11].
2. Energy Balance Based on Energy Intake and Energy Expenditure of Selected Obese Boys and Girls
. Details on the energy balance based on energy intake and energy expenditure of selected obese boys and girls are presented in Figure 1
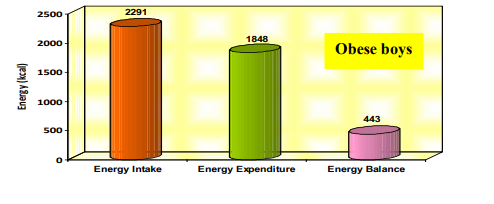
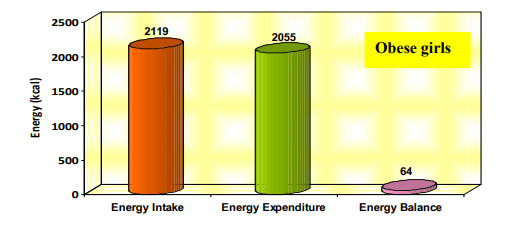
Energy intake of obese boys was found to be more than those of obese girls and the difference was significant (p<0.05). The energy expenditure was found to be more among obese girls when compared to obese boys which was also significant (p<0.05). Both boys and girls exhibited a positive energy balance which was higher in obese boys than in obese girls and the difference between them was found to be not significant. This can be attributed to increased energy intake and decreased energy expenditure among boys. Weight maintenance is largely a balance between the calories consumed through diet and those expended to support physical activity, for thermo genesis and to support basal physiologic function [12].
3. Mean Scores of Psychosocial and Behavioural Adjustment Problems
Table II presents the mean scores obtained for Psychosocial and Behavioural Adjustment Problems by the selected obese children.
Table II: Mean scores obtained for psychosocial and behavioural adjustment problems by the selected obese children
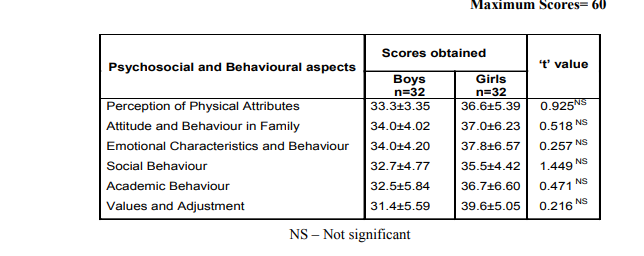
The findings revealed that none of the children scored lowest indicating that every obese child faced adjustment problems but not to a maximum extent. The difference in scores were found to be statistically not significant between obese boys and obese girls in all aspects .This observation may be because the selected children were in the school going age and not in the adolescent period where greater extent of adjustment problems are very common.
4. Biochemical profile of selected obese boys and girls
The biochemical profile of selected obese boys and girls is given in Table III.
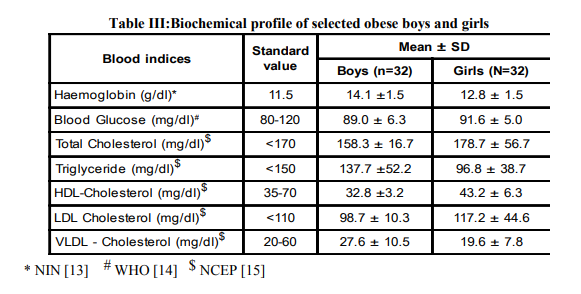
a. Haemoglobin levels
The mean haemoglobin values of both obese boys with 14.1g/dl and obese girls with 12.8 g/dl were above the normal value indicating that none of the selected children suffered from iron deficiency anaemia. A similar finding was observed in a study conducted at Pakistan on a total of 103 children (6-11 years) of which 74 per cent were obese and all the obese children had normal or above normal haemoglobin levels [16].
b. Blood glucose levels
It is observed from the table that the mean blood glucose level of both the obese boys (89mg/dl) and obese girls (91.6mg/dl) were within the normal range (80-120 mg/dl) indicating the absence of diabetes mellitus and impaired glucose tolerance among the selected obese children.
c. Lipid profile
The mean total cholesterol level of obese boys (158.3 mg/dl) was within the normal range but in the case of obese girls the level (178.7 mg/dl) was found to be slightly higher than the normal. The mean values of triglycerides were lesser than the normal values among both boys and girls with 137.7 mg/dl and 96.8 mg/dl respectively. HDL cholesterol level was found to be lower than the standard value for obese boys (32.8 mg/dl) whereas it was within the normal range for obese girls (43.2 mg/dl). LDL cholesterol values of obese boys (98.7 mg/dl) were within the normal value but it was higher than the standard value for girls (117.2 mg/dl). Mean VLDL cholesterol values for both obese boys and girls with 27.6 mg/dl and 19.6 mg/dl respectively were well within the normal values. It is evident from the table that total cholesterol and LDL cholesterol values of obese girls were slightly higher than the normal values compared to obese boys. In general, biochemical profile does not warrant any alarming diseases among the selected obese children.
5. Mean blood pressure of selected obese boys and girls
The mean blood pressure values of selected obese boys and girls are presented in Table IV.
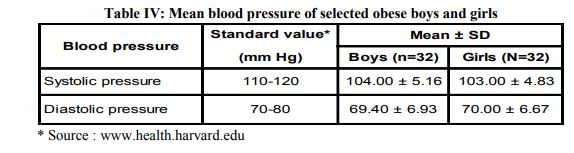
A study conducted on school children in India revealed that systolic or diastolic incident hypertension was found in 17.34 per cent of overweight children versus 10.1 per cent of remaining normal students (p<0.01) [17].Another study conducted at Ireland reported that obese boys (51%) and obese girls (49%) had initial blood pressure measurements in the hypertensive range. There was a correlation between the degree of obesity and systolic blood pressure, particularly in boys [18]. But in the present study, the systolic and diastolic pressures of both the obese boys and girls were found to be within the normal range and similar among both groups and the findings do not support some of the earlier studies.
CONCLUSION
Childhood obesity is one of the most serious public health challenges of the 21st century. The fundamental causes behind the increasing trend of childhood obesity include changing lifestyles of families, an increased intake of energy-dense foods and a trend towards decreased levels of physical activity. Overweight and obese children are likely to develop lifestyle diseases like diabetes mellitus and cardiovascular diseases at a younger age which is preventable. Prevention of childhood obesity therefore needs high priority. Lifestyles and behaviours are established at a young age. It is important for parents and children to focus on making longterm healthy lifestyle choices such as changing eating habits, increasing physical activity, engaging in a support group activity and setting realistic weight management goals.
ACKNOWLEDGEMENT
The authors extend their sincere thanks to the University Grants Commission, New Delhi for providing financial assistance to conduct this research. Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Flynn, D; Colecchia, A; Sacco, T; Bondi, M; Roda, E. and Marchesini, G. (2006), “Hepatic steatosis in obese patients clinical aspects and prognostic significance”, Obesity Review, Vol. 5, Pp. 27-42.
2. Stubbs, C.O. and Lee, A.J. (2004), “The Obesity Epidemic: Both Energy Intake and Physical Activity Contribute”, MJA, Vol.181, No.9, Pp. 489 - 491.
3. Speiser, P.W. Rudolf, M.C. and Anhalt, H. (2005), Childhood Obesity. J.Clin. Endocrinol Metab, 90: Pp.1871-1877.
4. Cornette, R. (2008). “The Emotional Impact of Obesity on Children”. Worldviews Evid Based Nurs 5 (3): 136–41.
5. Lau, D.C.W., Douketis, J.D., Morrison, K.M., Hramiak, I.M. and Sharma, A.M. (2007), “Canadian Clinical Practice Guidelines on the Management and Prevention of Obesity in Adults and Children (Summary)”, CMAJ, Vol.176, No.8, Pp. S1 - S13.
6. Swaminathan, M. Principles of Nutrition and Dietetics. Second Edition, Bapco Publishing, Bangalore, 2005. p.528.
7. Indian Council of Medical Research (ICMR). (2006), “Dietary Guidelines for Indians, Indian Council of Medical Research”, Hyderabad, Pp. 72 - 74.
8. Parik and Das, (1988), Secondary Handbook of Psychological and Social Instruments. Personality, Concept Publishing CO, New Delhi, Pp.70-75
9. Brion, M.A., Ness, A.R., Smith,G.D. and Leary, S.D. (2007), “Association Between Body Composition and Blood Pressure in a Contemporary Cohort of 9 Year Old Children”, J.Hum.Hyperten, Vol.21, Pp. 283 - 290.
10. Li, Y., Zhai,F., Yang, X., Schouten,E.G., Hu,X., He,Y., Luan,D. and Ma,G. (2007), “Determinants of Childhood Overweight and Obesity in China”, Brit.J.Nutr, Vol.97, Pp. 210 - 215.
11. Jennifer, L.B. and James, M. (2008) Neighborhoods and Obesity, Nutrition, Vol.66 (1), Pp.2-20.
12. National Institute of Nutrition (1990), “Techniques of Iron Status Measurement” Manual of Collection, Processing and Estimation of Samples for Iron and Iodine Status Measurements. National Institute of Nutrition, Hyderabad, India.
13. World Health Organisation (2003), Joint WHO/FAO Expert Consultation on Diet, Nutrition and the Prevention of Chronic Diseases. WHO Technical Report Series 916, Geneva, Switzerland.
14. National Cholesterol Education Programme (NCEP), 2005, Expert Panel on Blood Cholesterol in Children and Adolescents, Amer. Heart. Ass., 112, 3184-3209.
15. Ramzan, M., Ali, I. and Salam, A. (2009), Iron Deficiency Anemia in School Children of Dera Ismail Khan, Pakistan, Pakistan Journal of Nutrition, Volume: 8 Issue: 3, Page No.: 259-263
16. Manuraj, K. Sundaram, R. Paul, A. Deepa, S. Krishna Kumar R. (2007) Obesity in Indian children: Time trends and relationshipwith hypertension, The National Medical Journal of India vol. 20, No. 6.
17. Finucane, F. M., Pittock, S., Fallon, M., Hatunic, M., Ong, K. Burns, N. Costigan, C., Murphy. N. and Nolan J. J. (2008,) Elevated blood pressure in overweight and obese Irish children, Irish Journal of Medical Science, Volume 177, Number 4 , Pp.379-381
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





