IJCRR - 5(14), July, 2013
Pages: 69-76
Date of Publication: 29-Jul-2013
Print Article
Download XML Download PDF
COMPARATIVE STUDY OF PREVALENCE OF OCULAR MORBIDITY AMONG SCHOOL GOING CHILDREN OF GOVERNMENT AND PRIVATE SCHOOLS IN RURAL KARNATAKA, SOUTH INDIA
Author: Prasanna Kamath B.T, Girish M. Bengalorkar, B.S.Guru Prasad
Category: Healthcare
Abstract:Background: School children are affected by various eye disorders like refractive errors, squint, Vitamin A deficiency and eye infections. Children do not complain of defective vision. Uncorrected refractive errors form the primary cause for visual impairment and blindness in India. This warrants early detection and treatment of these problems to prevent future blindness. Aims: The study was conducted with the objective of comparing the prevalence of ocular problems among school going children studying at a government and a private school in rural area and to create 'eye-health awareness' among them. Method: This was a cross-sectional study of school children of two schools, one a government school and another private residential school in rural area of Karnataka state. The students were screened for eye disorders by visual acuity testing, anterior segment torch light examination and fundus examination with undilated pupil. Those children identified with ocular disorders were subjected for detailed examination at our tertiary care hospital. Results: A total of 700 children at government school and 600 among private school were examined. The prevalence of ocular morbidity was 74.29% among government school children and was only 10.33% among private school children. Vitamin A deficiency was conspicuously seen only among the government school children (62.7%). Refractive error was the commonest morbid condition among the private school children (6.5%). Conclusion: Ocular disorders among school going children can be easily identified by regular eye screening programmes, promptly treated can be protected from future complications and childhood blindness can be prevented.
Keywords: Eye screening, ocular disorders, refractive errors, rural area, school children.
Full Text:
INTRODUCTION
School health is an important aspect of any community health program. The school age is a formative period, physically as well as mentally, transforming the child into a promising adult. Health habits formed at this age will be carried to adult age, old age and even to the next generation. Poor vision in childhood affects performance in school and has negative influence on the future life of the child. Integration of vision screening and refractive services for school student with screening for health issues is recommended by World Health Organization.1,2 The relationship between scholastic performance and health status of children, in particular eye health is well established. School children are affected by various eye disorders like refractive errors, squint, Vitamin A deficiency and eye infections. Uncorrected refractive errors form one of the important causes of visual impairment and blindness in most developing countries including India. This along with Vitamin A deficiency forms a major preventable cause of blindness in the young age group i.e. <20years. Considering the fact that 30% of India’s blind lose their sight before the age of 20years, the importance of early detection and treatment of ocular morbidity and visual impairment in young children is obvious.3 Children do not complain of defective vision, and may not even be aware of the condition. They try adjusting to the problem of defective vision by sitting in the front benches, holding the books close to their eyes, squeezing the eyes. The earliest signs of refractive errors are strainful eyes with or without redness by evening, with watering and headache. These complaints of the child to the parents go unnoticed due to lack of awareness, more so among the children studying at a government school in the rural areas. This warrants early detection and treatment of ocular problems to prevent future blindness. Effective methods of vision screening in school children are useful in detecting correctable causes of decreased vision, especially refractive errors.4 School children form a sizeable segment of the community. Children in school going age group (6-15years) represent 25% of the population in developing countries5 . They are easily accessible and schools are the best forum for imparting health education to the children. Schools are also one of the best centres for effectively implementing the comprehensive eye health care programme4 . The importance of visual acuity was identified for the first time in United States during Second World War6 and in India; Mukherjee et al 7 stated the importance of early detection and treatment of refractive errors to prevent permanent disability. Magnitude and causes of uncorrected refractive errors differ in the urban and rural areas of India. Therefore refractive eye services are to be modified according to the situation in various areas of developing countries.8 The eye problems happen to go undetected and untreated among the government schools. More over data about these ocular problems are not available in this rural part of our country. Hence the study was conducted with the primary objective of comparing the prevalence of ocular problems among government and private school children in rural area, secondarily to provide appropriate treatment and also to create ‘eyehealth awareness’ among school children in rural area.
MATERIALS AND METHODS
Study Sample: Two schools were selected randomly of the six schools in the field practice area of Department of Community Medicine, Sri Devaraj Urs Medical College, Kolar. The government school had student strength of 715 and the other a private school had 605 students, both in rural areas. Study Setting: All the students in the two schools were included in the study considering the absentees on the days of examination. The principals and teachers of the schools were informed and explained about the study and permission for the visit was obtained in advance. Official written permission to conduct study was also taken. The principals in turn communicated to the parents and written consent was taken in their school diaries. They were ensured strict confidentiality and informed consent was taken from each participant. Design: It was a cross sectional study in two stages. In the first stage the general data regarding the age, gender, address, parents, was collected using a pre-tested structured questionnaire. Information was obtained from the children in the local language and entered in English language in the questionnaire. The students were screened for eye disorders by visual acuity testing, anterior segment torch light examination and fundus examination with undilated pupil. Visual acuity was assessed using Snellen’s chart; color blindness was checked by using Ishihara’s chart. Vitamin A deficiency was diagnosed if there was history of night blindness, or on examination there were signs of conjunctival xerosis, Bitot’s spots, corneal xerosis, or keratomalacia. Examinations were performed in the schools. All the children present at the time of visit were examined. Those children absent were informed about the same and made to undergo examination on a scheduled day. This eye screening was performed at the school itself by the doctors who were trained with the requisite skills by an eye specialist (ophthalmologist) at our hospital. In the second stage those children identified with ocular disorders were subjected for detailed examination at our tertiary care hospital by specialists on a scheduled day for further evaluation, classification and quantification of types of ocular problems, appropriate medical treatment and suitable spectacle correction. The data was analyzed using Epi Info. The chisquare test was used to test differences in proportions. The difference was considered to be statistically significant if p value was <0.05.
RESULTS
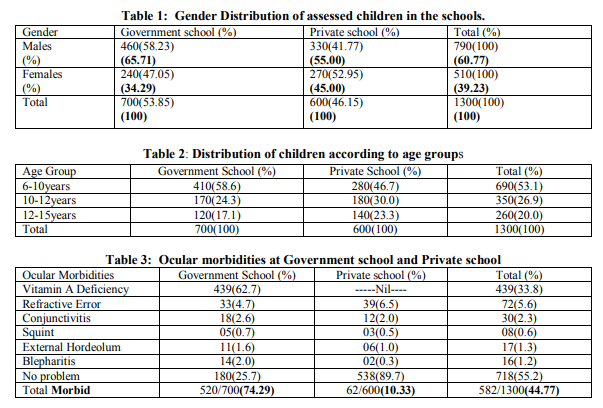
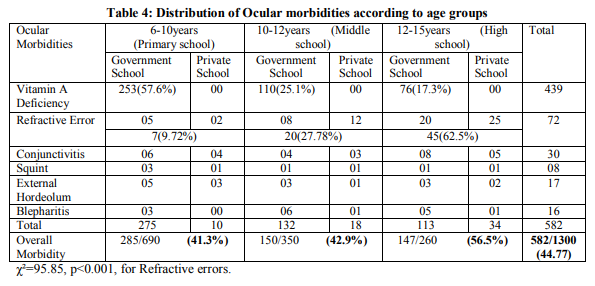
A total of 1300 children (20 students were absent in spite of our persistent efforts) were examined for ocular morbidity belonging to two schools. Table 1 shows the gender distribution of the study population. The overall proportion of boys (60.77%) was more compared to that of girls (39.23%). Boys and girls were more equally distributed among the private school (55% to 45%) as compared to the government school (65.71% to 34.29%). Table 2 shows that the proportion of children in younger age groups was more compared to older age groups, which was observed to be the same in both the schools. Table 3 shows proportion of ocular morbidity among study population. Vitamin A deficiency was the chief morbidity among the children (33.8%) followed by refractive errors (5.6%) and conjunctivitis (2.3%). The least problem was squint of 0.7%. Here the notable difference was that Vitamin A deficiency was seen only in the government school students and the prevalence was 62.7%. The refractive error was the commonest problem among the private school going children (6.5%) and all of them were detected and treated. While refractive error among the government school children was to the extent of 4.7% and none of them were detected and treated. Table 4 shows that ocular morbidity was least among primary school children (41.3%) followed by middle school and high school children with 42.9% and 56.5% respectively. Vitamin A deficiency was highest in the primary school children (57.3%) and least among high school children (17.3%).This difference was found to be not statistically significant. On the contrary refractive error increased as age increased i.e. 9.72% among primary school, 27.78% among middle school and a maximum of 62.50% among high school children. This was highly significant statistically (χ²=95.85, p<0.001). This proportionate increase in the prevalence of refractive error was seen among both the government and private school children. Middle school children were least affected with conjunctivitis and external hordeolum. Refractive errors were slightly more among the boys (55.56%) as compared to girls (44.44%). This difference was not statistically significant.
DISCUSSION
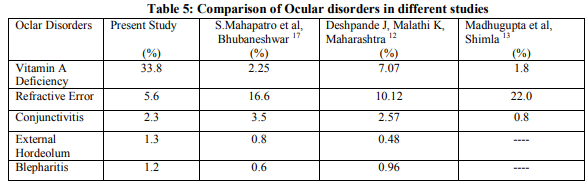
The present study shows high prevalence of ocular morbidity among school children in rural areas. This shows the need to implement the eye checkup compulsorily in the school health appraisal programme. In the present study, prevalence of ocular morbidity was 44.77% comparable to the one reported by Chaturvedi et al (more than 40%) in rural Delhi9 and Kalikivayi et al (43.5%) at Hyderabad10 but a lower prevalence was reported by Rajesh Kumar et al (24.6%) from Delhi11 , Jayanth D and Malathi K (27.65%) from rural Maharashtra12 and Madhu Gupta and others (31.6%) from Shimla13. Least prevalence of 13% was reported by Prajapati P et al among adolescents of Gandhinagar district3 and 15.6% by Wedner SH et al in rural Tanzania 14. The prevalence of ocular morbidity varies at different places due to different factors prevailing at different places. Vitamin A deficiency was the commonest ocular morbidity (33.8%) which manifested as bitot spots and conjunctival xerosis. In a study at rural north Mahrashtra by Jayant D and Malathi, 25.58% Vitamin A deficiency was reported 12 and 29.3% was noted by Prajapati et al at Gandhinagar3 . Mausami Basu et al reported 11.83% of conjunctival xerosis among students at Surat15 and Bhattacharya et al observed 8.16% Vitamin A deficiency among primary school students in Darjeeling district16 but S.Mahapatro et al noted least prevalence 2.25% Vitamin A deficiency in Bhubanesar17 . In the present study Vitamin A deficiency was more among primary school children and decreased as they reached high school. This was probably due to better eating habits as the child grew up. The reason for high prevalence of Vitamin A deficiency in our study may be that the study was done in rural area where majority of them belonged to low socioeconomic status and also under nutrition was seen. Vitamin A deficiency manifestations in eye were more among girls as compared to boys which was highly significant statistically (p<0.001). This may be due to the fact that male children are given more importance with respect to diet in terms of types of food given. Uncorrected refractive error was the second common morbid condition (5.6%) among the children comparable to the study by Jayant D and Malathi K in rural Maharashtra12 and S Mahapatro et al at Bhubanesar17. Madhu Gupta et al at Shimla had identified refractive error as the commonest morbidity among children (22%) 13 in their study and Prajapati et al also had observed it as the commonest with a prevalence of 40.1% in their study at Gandhinagar3 . Higher prevalence of refractive error of 32% has been reported by Kalikivayi in a study from South India10 and 61% among children in rural population of India by Dandona R et al18. In a study at Pune among adolescent school children Col A Datta et al noted 21.19% of refractive error19 . In our study refractive error increased with age and this was statistically significant. Similar pattern has been noted by S Mahapatro et al at Bhubanesar17 and also by Goh PP et al in Malaysia20. Screening for refractive errors is an integral part of School health problem. Unfortunately it is not taken seriously and children suffering with refractive errors are still high. Prevalence of conjunctivitis was 2.3% in our study, similar to the one reported by Jayant D and Malathi K (2.57%) at rural Maharashtra12 , but more than that studied in Shimla (0.8%) by Madhu Gupta et al13 and less than that by Prajapati (3.8%) et al at Gandhinagar3 , and Kumar R et al (4.6%) in urban and rural Delhi21 . This high prevalence may be explained by the fact that most of the children were from lower socioeconomic status and so more likely for the poor personal hygiene. Table 5 shows the comparison of the prevalence of different ocular morbidities in our study and other studies at different places. Prevalence of Vitamin A deficiency was significantly high in our study and that was seen only among the government school children and this could be due to the fact that the students in the government school belong to lower socio economic status and our area is one of the most backward areas in the country. Prevalence of refractive errors was least among the various studies and this may be because the children did not have risk factors like reading in badly illuminated areas, over exposure to television or the computers due to their rural background. Conjunctivitis was similar in other studies but for that conducted at Shimla which is an urban area.12, 13, 17 The study showed an increase in morbidity with age. This may be due to the fact that the dropout rate from school was high due to poverty, and refractive error related to habits like prolonged study hours, watching television bad reading posture increased and hygienic practice related problems like blepharitis, external hordeolum also increased.
CONCLUSION
The study clearly indicates the prevalence of ocular morbidity among school going children in rural Karnataka, India is high. Vitamin A deficiency and refractive errors are the most common ocular disorders identified which are the preventable and treatable causes of childhood blindness and visual impairment identified by the World Health Organization under Vision 2020 programme. The undetected refractive errors are seen in the government school children and need to be provided with corrections and regular follow up. Both these conditions can be easily identified by regular eye screening programmes and promptly treated so that the future citizens of our country are protected from becoming blind. The awareness among school teachers should also be improved and they should play an active role in identifying the ocular problems and referring them for timely management. Lastly, it is high time that we identify one month in a year and designate it as “Child’s Eye Health and Safety Month” to conduct eye screening for morbidities among school children, their management and to spread awareness regarding Eye Health. In India importance is given when a program is conducted in a campaign mode, but when it is integrated into regular health services the programme loses its importance. A strict monitoring of school health programme has to be implemented with accountability and suitable action needs to be taken.
ACKNOWLEDGEMENTS
We would like to thank the heads of the institution, the teachers and more so the students for having been very co-operative in the collection of the data. We thank our entire department faculty for being encouraging and supportive throughout this study. Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Name of Ethical Committee-Institutional Ethics Committee of Sri Devaraj Urs Medical College, Kolar, Karnataka, India
References:
1. Elimination of avoidable visual disability due to refractive error. Report of an informal planning meeting WHO/PBL/00.77.Geneva;WHO;2000WHO; 6-10
2. Health dialogue: A forum for the exchange of news and views on primary health care in India.Inveno. 2006;44:1
3. Prajapati P, Oza J, Prajapati J, Kedia G, Chudasama RK. Prevalence of Ocular morbidity among school adolescents of Gandhinagar district, Gujrat. Online J Health allied Scs.2010;9(4):5
4. Danish Assistance to the National Programme for control of Blindness. New Delhi, India: Vision screening in school children. Training module 1.
5. World Health Organization (1999) Report of WHO/IAPB scientific meeting, Hyderabad, India 13-17th April. Childhood Blindness Prevention. WHO/PBL/87 6. Davens E. The nationwide alert to pre-school vision. Screening sight saving review 1966;1:180-4.
7. Mukherjee R, Seal SC. An epidemiological study of refractive errors among school children in Calcutta. JIMA 1973.73:59-64
8. Padhya AS, Khandekar R, Dharmadhikari S, Dole K, Gogate P, Deshpande M. Prevalence of uncorrected refractive errors and other eye problems among urban and rural school children. Middle East Afr J Ophthalmol 2009;16:69-74
9. Chaturvedi S, Aggarwal OP. Pattern and distribution of ocular morbidity in primary school children of rural Delhi. Asis Pac J Public Health.1999;11(1):30-3.
10. Kalikivayi V, Naduvilath TJ, Bansal AK, Dandona L. Visual Impairment in school children in Southern India. Indian J Ophthalmol.1997;45:129-34
11. Kumar R, Dabas P, Mehra M, Ingle GK, Saha R , Kamlesh. Ocular morbidity among primary school children in Delhi. Health and population-perspective and issues.2007;30(3):222-229
12. Deshpande Jayant D, Malathi K. Prevalence of ocular morbidities among school children in rural area of North Maharashtra in India. National Journal of Community Medicine.2011 July-Sept;Vol2 Iss2:249-254
13. Gupta M, Gupta BP, Chauhan A, Bhardwaj A. Ocular morbidity prevalence among school children in Shimla, Himachal, North India. Indian Journal of Ophthalmology.2009 Mar-Apr;57(2):133-138
14. Wedner SH, Ross DA, Balire R, Kaji L, Foster A. Prevalence of eye diseases in primary school children in a rural area of Tanzania. Br J Ophthalmol.2000;84:1291- 7[PMCID:PMC1723290][PubMed:11049957 ].
15. Mausami Basu, Palash Das, Ranabir Pal, Sumit Kar, Vikas K Desai and Abhay Kavishwar. Spectrum of visual impairment among urban female school students of Surat. Indian J Ophthalmol.2011 NovDec;59(6):475-479
16. Bhattacharya RN, Shrivastava P, Sadhukhan SK, Lahiri SK, Chakravorty M, Saha JB, et al. A study on visual acuity and vitamin A deficiency among primary school students in Naxalbari village, Darjeeling district of West Bengal. Indian J Pub Health.@04;48:171-180
17. S Mahapatro, MK Das, GK Padhy, SS Kar, AK Nanda. Prevalence of ocular disorders in school children in rural area surrounding Bhubanesar. Journal of Community Medicine.2010 Jan-June;Vol6(1)
18. Dandona R, Dandona L, Srinivas M, Sahare P, Narsaiah S, Munoz SR, Pokharel GP, Ellwein LB. Invest Ophthalmol Vis Sci.2002 Mar;43(3):615-22
19. Col A Datta, Lt N Bhardwaj, SR Patrikar, Col R Bhalwar. Study of disorders of visual acuity among adolescent school children in Pune. MJAFI.2009;65:26-29
20. Goh PP, Abqariyah Y, Pokharel GP, Ellwein LB. Refractive error and visual impairment in school-age children in Gombak district, Malaysia. Ophthalmology.2005;112:678-85.
21. Kumar R, Mehra M, Dobas P, Kamlesh, Raha R. A study of ocular infections amongst primary school children in Delhi. Indian J Commun Dis.2004;36:121-26
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





