IJCRR - 8(5), March, 2016
Pages: 22-26
Date of Publication: 13-Mar-2016
Print Article
Download XML Download PDF
CLINICOCYTOLOGICAL ANALYSIS OF CYSTOSARCOMA PHYLLOIDES VIS A VIS FIBROADENOMA
Author: Brij Mohan Kumar Singh, Arijit Bishnu, Varun Kumar Singh
Category: Healthcare
Abstract:Aim: Phyllodes (PT) tumor is a rare fibro-epithelial neoplasm but requires an accurate preoperative diagnosis on fine needle aspiration cytology and most importantly to be distinguished from fibroadenoma, which allows the surgeon for correct surgical planning and avoidance of reoperation. We have evaluated both these neoplasm and tried to draw a distinction line between these two entities. Methodology: The archival files of department of pathology, Kasturba Medical College, Manipal were searched and cases which were confirmed on histopathology as benign phyllodes were retrieved. For comparison cytologically diagnosed and histopathologically confirmed cases of fibroadenoma were taken. The cytological material in all cases consisted of alcohol fixed Papanicolaou-stained smears. Cytological features of their epithelium and stromal component constituting the background dispersed cell population were evaluated in detail. Results: The number of epithelial fragments including both cluster and syncytial architecture with apocrine metaplasia along with highly cellular and regular borders of stromal fragments and increased numbers of long spindle nuclei to other background nuclei in phylloides tumour were found informative Conclusion: The rate of picking up of these entities on FNA would increase by following these general guidelines and will also add up in good reproducibility.
Keywords: Cystosarcoma phylloides, Fibroadenoma, Fine needle aspiration cytology
Full Text:
INTRODUCTION Phyllodes tumor (PT) also known as cystosarcoma phylloides are typically large, fast growing masses that originates from the periductal stromal cells of the breast. They are rare fibroepithelial neoplasm and accounts for less than 1% of all breast tumour1 . These tumours are often misdiagnosed by the pathologist leading to partial treatment by the surgeon. Thus, pose a great challenge in the preoperative diagnosis to allow correct surgical intervention and avoid reexploration. During the clinical evaluation, age of the patient may give some clues but should never be overemphasized. These tumours may have identical clinical and radiological features.2 Cytologically, problem gets intensified, as both these tumors, Phylloides and Fibroadenoma(FA) share many features.
Most of the time diagnosis of malignant phylloides is straight forward because of the presence of obvious anaplasia. Problem arises when we have to distinguish between low grade phylloides and fibroadenoma on FNA (Fine needle aspiration cytology). In various studies the cytological features of PT have been described in great details, but the entity in the grey-zone areas i.e. benign variant of PT have not been given enough emphasis in the literature. The study was undertaken to try and evaluate the cytological features of phyllodes tumor with special reference to features that can help in distinguishing it from fibroadenoma.
MATERIALS AND METHOD The archival files of department of pathology, Kasturba Medical College, Manipal were searched from 2007 to August 2015.44 cases of phyllodes tumor diagnosed on FNA were retrieved.Only 24 cases were confirmed on histopathology as benign phyllodes .These 24 cases were considered for the study; FNA slides of the same were reviewed and assessed. The comparison group consisted of 68 cytologically diagnosed and histopathologically confirmed cases of fibroadenoma.The cytological material in all cases consisted of alcohol fixed Papanicolaou-stained smears.
Cytological features of their epithelium and stromal component constituting the background dispersed cell population were evaluated in detail. ? Epithelial cell cluster were studied for the following features ? Number and architecture of the clusters ? Stromal fragments were assessed for ? Number and cellularity of fragments. ? Cellularity was graded as 1+,2+, and 3+ ? Blood vessel crossing the fragments ? The background stromal cells were also studied in details and the cellularity was graded as 1+, 2+ and 3+ ? Characteristics of dispersed cells were studied and the percentage of spindle cells noted. ? Size and shape of the individual dispersed cell were studied and graded as ? Big( when cell size is more than 2 times the small lymphocyte) ? Small (when the size is less than small lymphocyte.)
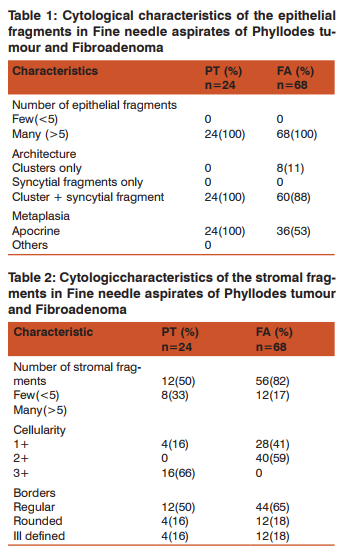
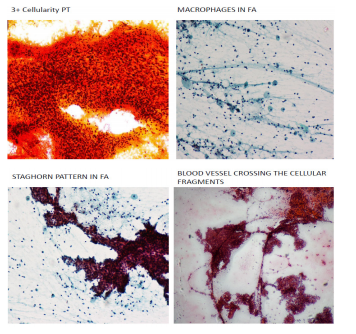
RESULTS Both the tumour group were characterized by dimorphic pattern. All the cases of both phylloids and fibroadenoma showed many epithelial fragments with 8 cases of fibroadenoma showed only cluster (Table1). There were not many differences in the epithelial features among the two tumour group. More amount of epithelial cells seen in FA as compared to PT. most of the cases of FA showed monolayered sheets of epithelial with staghorn branching pattern and variable number of bare nuclei in the background. Apocrine metaplasia was noted in all the cases of phylloides tumour. The number of stromal fragments was more in number seen in cases of phylloides tumour as compared to fibroadenoma.
The stromal fragments in both the groups were variable in shape, but were cellular and many having myxoid appearance in cases of phylloides tumour. (Table2) The background elements in both the groups showing 3+ and 1+ cellularity in PT and FA respectively. Majority of the phylloides tumour show big cellular architecture with long spindle shaped cells, whereas fibroadenoma showed small sized cells with round architecture. (Table3) Majority of the FA showed foam cells in the background. Considering the background of the smear we saw majority of the phylloides tumour is composed of long spindly nuclei as compared to the fibroadenoma group. (Table 4) Majority of the FA cases shows thin walled blood vessel crossing the epithelial and stromal fragments. (Table5)

DISCUSSION Phyllodes tumour are given as diagnosis on the FNAC when a cytologist see numerous hypercellular stroma and the stromal elements than the epithelial component on the smears. The cells on thesmears were classified by Deen SA et al3 in 1999, and Jayaram G and Sthaneshwar P in 20024 , by comparison with small lymphocytes, in: 1. Short, round/oval cells, two-size smaller than the size of a lymphocyte : considered to be epithelial cells 2. Long, spindle cells, three-size larger than the size of a lymphocyte:considered to be stromal cells.
Phyllodes tumour are further categorized as benign, borderline, or malignant based on certain features such as margins of the tumour, amount of stromal overgrowth, cellularity, necrosis, pleomorphism, and the mitotic figure per high-power field5 generally the treatment protocol for the phyllodes tumour is wide excision because of their inherent property of local recurrence. It has been also suggested in various studies that grades of phyllodes tumour has poor correlation with the local recurrence6,7 but, a well-established relationship has been proved for their metastasis8 therefore there is no room for underdiagnosis by pathologist and overtreatment by the surgeon or vice-versa.
Identification of malignant phyllodes tumors do not pose great challenge as is seen in cases of benign and borderline phyllodes tumors which bear great resemblance to, and are usually mistakenly diagnosed as, fibroadenoma. Such problem are generally seen even with the experienced eye when the stromal component is the dominant component on FNA with marked atypia, pleomorphism and high mitotic activity.9, 10
We, in the present study tried to compare the fibroadenoma and phyllodes tumour on the basis of epithelial and stromal fragment along with the background nuclei in conjunction with Bandyopadhyay, et al11 Most of the studies done on cytological features of the two entities were based on ? Stroma, including the presence of hypercellular stromal fragments, ? Cellularity of the background nuclei, ? Cellular composition and morphology of background nuclei. Many studies have compared the cytomorphology of phyllodes tumor with fibroadenoma and these have yielded conflicting results.12, 13
The presence of hypercellular stromal fragment is the most useful feature in distinguishing phyllodes tumor from fibroadenoma.Hypocellularity of stromal fragments have been noted in both benign phyllodes tumor and Fibroadenoma.14 Similarly, as found by R Bandhyopadhyay et al11, in our study also the stromal fragments found to be hypercellular with more well defined regular borders in phyllodes tumor, compared to Fibroadenoma, with few exceptions.Study done by krisnamurthy et al7 , Suggests that in the event of hypercellular stromal fragments in fibroadenomas, the degree of background cellularity, composition and proportion of long spindly cells may be useful features in differentiation.
Our study has also shown that most of the phyllodestumors have 3+ cellularity of the background nuclei as compared to 1+ in most cases of Fibroadenoma.Size of the background cells also play an important role in cases of phyllodes tumor as most of them have bigger size cells as compared to smaller size in Fibroadenoma.In comparison to study by Nina S. Shabb et al15, Foamy macrophages are not seen in any cases of phyllodes tumor whereas 41% of the Fibroadenoma cases shown this feature.
The importance of spindle cells in the dispersed cell population has been emphasized by some workers16, and we found it to be useful in our study too.While studying these parameters individually may not give encouraging results, taken together, they can be used effectively in distinguishing these two groups of tumor. Based on the stromal fragment an algorithm can be given to guide for differentiating these two dubious entities.

CONCLUSION The preoperative diagnosis and proper management is crucial in Phyllodes tumor. Both Phyllodes tumor and fibroadenoma share many features in common as seen in this study as epithelial characteristic on the FNA smears. The savior in these cases would be to consider the high cellularity, long spindly cell architecture with numerous spindly nuclei in the background with reduced number of blood vessel crossing the epithelial and stromal fragments. FNA has proven to be very reliable and fairly reproducible by choosing the above mentioned feature in differentiating between PT and FA.
ACKNOWLEDGEMENT Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Source of Funding Authors will bear all the expenses towards this research work. Conflict of interest: None
References:
1. Jacklin RK et al. optimising preoperative diagnosis in phyllodes tumor of breast. J clin pathol 2006; 59:454-9
2. David D et al. Fine needle aspiration cytology of phyllodes tumor- potential diagnostic pitfalls. 1992;36:215-21
3. Deen SA, McKee GT, Kissin MW. Differential cytologic features of fibroepithelial lesions of the breast.Diagnostic Cytopathol 1999;20:53–6.
4. Jayaram G, Sthaneshwar P. Fine-needle aspiration cytology of phyllodes tumors. Diagn Cytopathol. 2002 Apr;26(4):222-7.
5. Tavassoli FA, Devilee P. Fibroepithelial Tumours. In Tavassoli FA, Devilee D eds. WHO Classification of Tumours: Tumours of the Breast and Female Genital Organs. Lyon: IARC Press; 2003:99-103.
6. Kok KY, Telsinghe PU, Yapp SK. Treatment and outcome of cystosarcoama phyllodes in Brunei: a 13-year experience. J R Coll Surg Edinb. 2001;46:198-201.
7. Kario K, Maeda S, Mizuno Y, Makino Y, Tankawa H, Kitazawa S. Phyllodes tumours of the breast: a clinicopathological study of 34 cases. J Surg Oncol. 1990;45:46-51.
8. Moffat CJ, Pinder SE, Dixon AR, Elston CW, Blamey RW, Ellis IO. Phyllodes tumour of the breast: a clinicopathological review of 32 cases. Histopathology. 1995; 27:205-218.
9. Jayaram G, Sthaneshwar P. Fine needle aspiration cytology of phyllodes tumour. Diagn Cytopath. 2002;26:222-227.
10. Shabb NS. Phyllodes tumour. Fine needle aspiration cytology of 8 cases. Acta Cytol. 1997;41:21-26.
11. R Bandhyopadhyay et al . Distinction of phyllodes tumor from fibroadenoma: cytologists perspective. Journal cytology 2010;27:59-62.
12. Dusenbery D et al. Fine needle aspiration cytology of phyllodes tumor. Potential diagnostic pitfalls. Acta cytol.1992;36:215-21.
13. Shimizu K et al. Cytologic evaluation of phyllodes tumors as compared to Fibroadenoma of the breast. Acta cytol 1994;38:891-7
14. Scolyer RA et al. Can phyllodes tumor of breast be distinguished from fibroadenoma using fine needle aspiration cytology. Diagnostic pathology. 2001;33:437-43.
15. Shabb NS et al. Phyllodes tumor.Fine needle aspiration cytology of eight cases. Acta cytol 1997;41:321-6
16. Rao CR Cystosarcoma phyllodes, diagnosis by fine needle aspiration cytology. Acta cytol. 1992;36:203-7.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





